

Portal vein embolization before liver resection: a systematic review
- PMID: 22806245
- PMCID: PMC3549243
- DOI: 10.1007/s00270-012-0440-y
Portal vein embolization before liver resection: a systematic review
Abstract
Purpose: This is a review of literature on the indications, technique, and outcome of portal vein embolization (PVE).
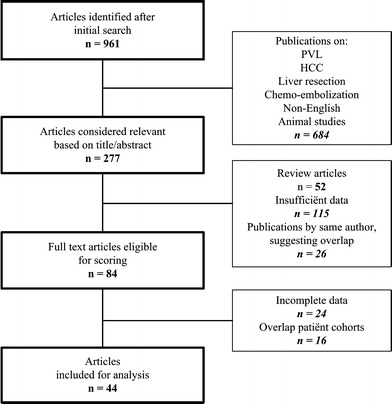
Methods: A systematic literature search on outcome of PVE from 1990 to 2011 was performed in Medline, Cochrane, and Embase databases.
Results: Forty-four articles were selected, including 1,791 patients with a mean age of 61 ± 4.1 years. Overall technical success rate was 99.3 %. The mean hypertrophy rate of the FRL after PVE was 37.9 ± 0.1 %. In 70 patients (3.9 %), surgery was not performed because of failure of PVE (clinical success rate 96.1 %). In 51 patients (2.8 %), the hypertrophy response was insufficient to perform liver resection. In the other 17 cases, 12 did not technically succeed (0.7 %) and 7 caused a complication leading to unresectability (0.4 %). In 6.1 %, resection was cancelled because of local tumor progression after PVE. Major complications were seen in 2.5 %, and the mortality rate was 0.1 %. A head-to-head comparison shows a negative effect of liver cirrhosis on hypertrophy response. The use of n-butyl cyanoacrylate seems to have a greater effect on hypertrophy, but the difference with other embolization materials did not reach statistical significance. No difference in regeneration is seen in patients with cholestasis or chemotherapy.
Conclusions: Preoperative PVE has a high technical and clinical success rate. Liver cirrhosis has a negative effect on regeneration, but cholestasis and chemotherapy do not seem to have an influence on the hypertrophy response. The use of n-butyl cyanoacrylate may result in a greater hypertrophy response compared with other embolization materials used.
Figures
References
-
- Honjo I, Kozaka S. Extensive resection of the liver in two stages. Rev Int Hepatol. 1965;15:309–319. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
