

What is the best way to apply the Spurling test for cervical radiculopathy?
- PMID: 22806265
- PMCID: PMC3830095
- DOI: 10.1007/s11999-012-2492-3
What is the best way to apply the Spurling test for cervical radiculopathy?
Abstract
Background: A diagnosis of cervical radiculopathy is based largely on clinical examination, including provocative testing. The most common maneuver was described in 1944 by Spurling and Scoville. Since then, several modifications of the original maneuver have been proposed to improve its value in the diagnosis of cervical radiculopathy.
Questions/purposes: We assessed the ability of six known variations of the Spurling test to reproduce the complaints of patients diagnosed with cervical radiculopathy.
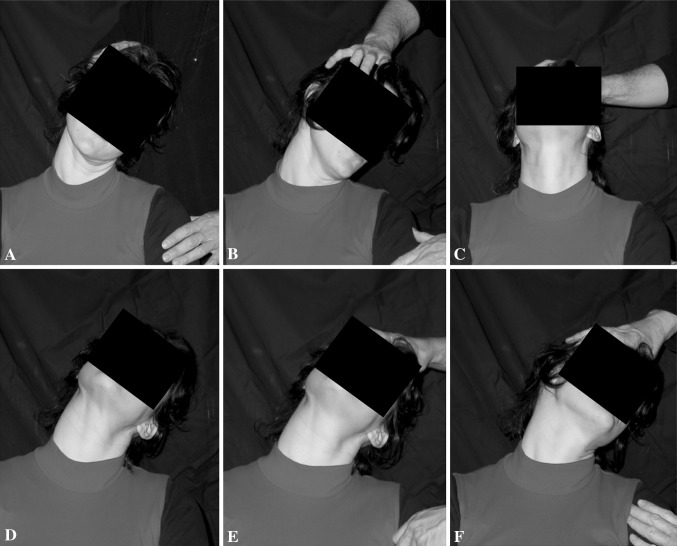
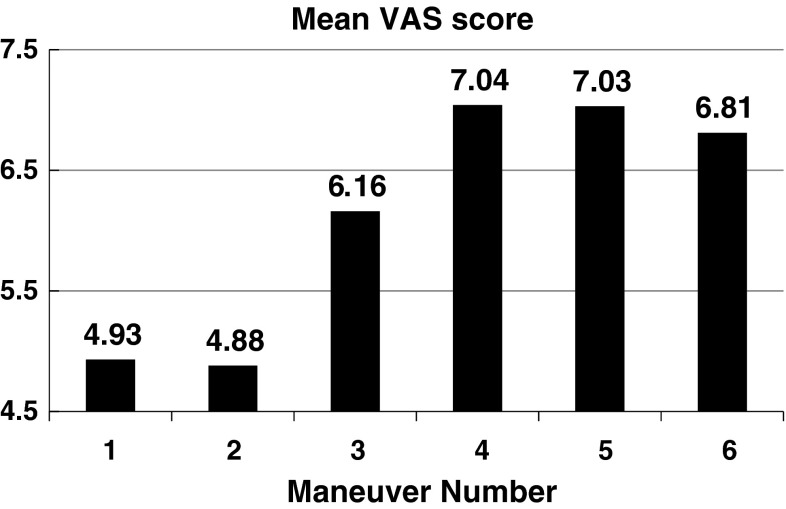
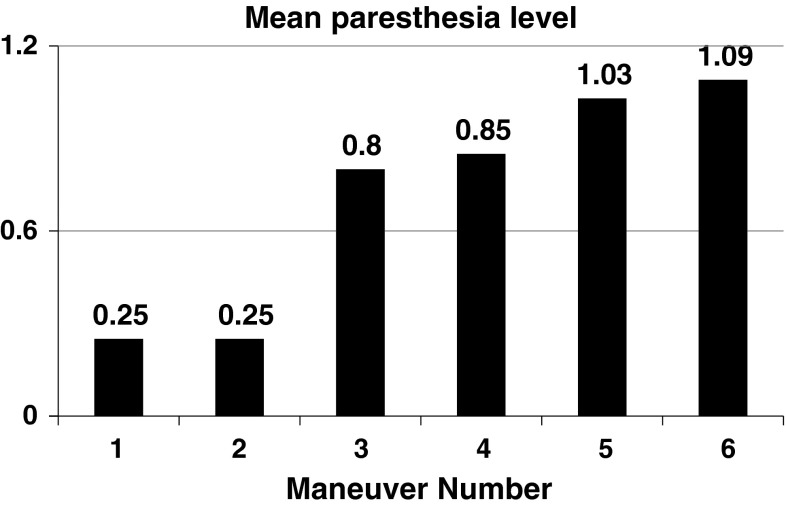
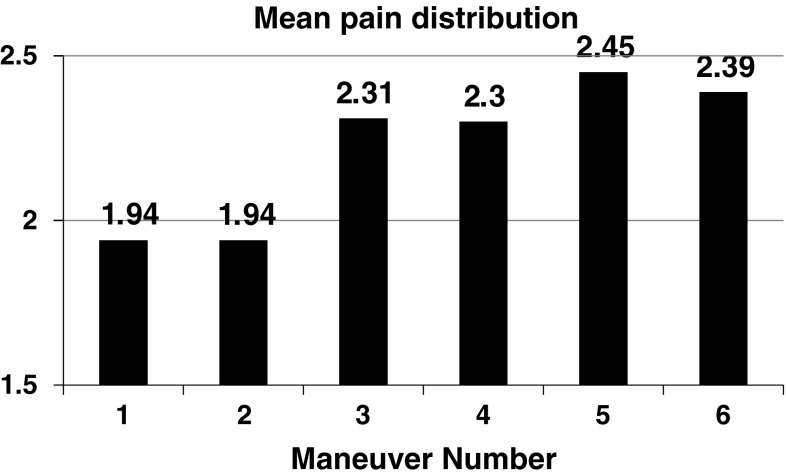
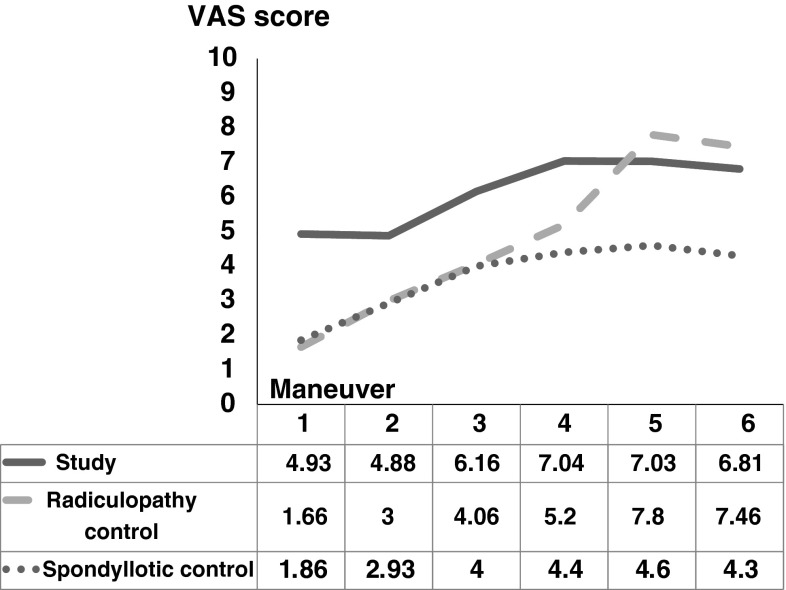
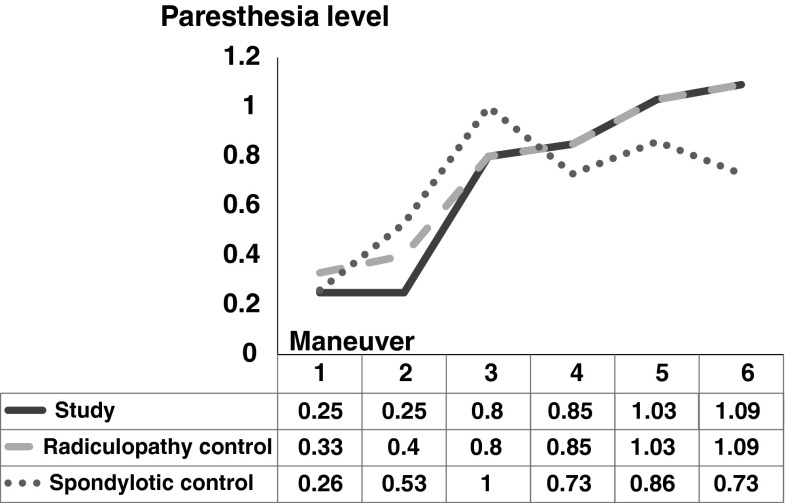
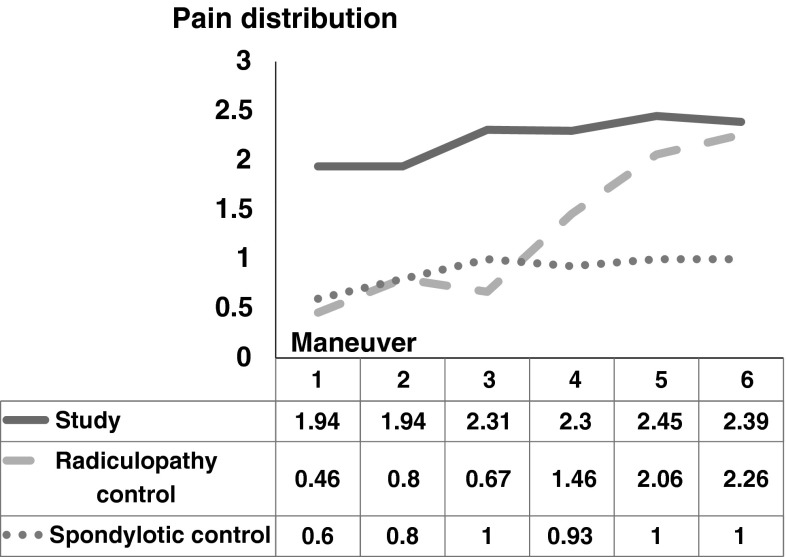
Methods: We prospectively enrolled 67 patients presenting with cervical radicular-like symptoms and concordant radiographic findings. Each patient underwent six distinct provocative cervical spine maneuvers by two examiners, during which three parameters were recorded: (1) pain intensity (VAS score), (2) paresthesia intensity (0 - no paresthesia, 1 - mild to moderate, and 2 - severe), and (3) characteristic pain distribution (0 - no pain, 1 - neck pain only, 2 - arm pain only, 3 - pain elicited distal to the elbow). The interobserver reliability of the reported VAS score (measured by the intraclass coefficient correlation) ranged from 0.78 to 0.96 and the calculated kappa values of the categorical parameters ranged from 0.58 to 1.0 for paresthesia intensity and from 0.63 to 1.0 for pain distribution. Differences in scores elicited between the two examiners for the 67 patients were resolved by consensus.
Results: A maneuver consisting of extension, lateral bending, and axial compression resulted in the highest VAS score (mean, 7) and was associated with the most distally elicited pain on average (mean, 2.5). The highest paresthesia levels were reported after applying extension, rotation, and axial compression (mean, 1). These maneuvers, however, were the least tolerable, causing discontinuation of the examination on three occasions.
Conclusions: Whenever cervical radiculopathy is suspected our observations suggest the staged provocative maneuvers that should be included in the physical evaluation are extension and lateral bending first, followed by the addition of axial compression in cases with an inconclusive effect.
Figures
Similar articles
-
Diagnostic Accuracy of the Neck Tornado Test as a New Screening Test in Cervical Radiculopathy.Int J Med Sci. 2017 Jun 23;14(7):662-667. doi: 10.7150/ijms.19110. eCollection 2017. Int J Med Sci. 2017. PMID: 28824298 Free PMC article.
-
Evaluation of Cervical Vertebral Motion and Foraminal Changes During the Spurling Test Using Zero Echo Time Magnetic Resonance Imaging and Computed Tomography-Based Micromotion Analysis.Spine (Phila Pa 1976). 2024 Jul 15;49(14):E221-E228. doi: 10.1097/BRS.0000000000005010. Epub 2024 Apr 9. Spine (Phila Pa 1976). 2024. PMID: 38595107
-
The Spurling test and cervical radiculopathy.Spine (Phila Pa 1976). 2002 Jan 15;27(2):156-9. doi: 10.1097/00007632-200201150-00007. Spine (Phila Pa 1976). 2002. PMID: 11805661
-
Evaluation of persons with suspected lumbosacral and cervical radiculopathy: Electrodiagnostic assessment and implications for treatment and outcomes (Part I).Muscle Nerve. 2020 Oct;62(4):462-473. doi: 10.1002/mus.26997. Epub 2020 Jul 18. Muscle Nerve. 2020. PMID: 32557709 Review.
-
Cervical radiculopathy.Med Clin North Am. 2014 Jul;98(4):791-9, xii. doi: 10.1016/j.mcna.2014.04.001. Med Clin North Am. 2014. PMID: 24994052 Review.
Cited by
-
The Spine Physical Examination Using Telemedicine: Strategies and Best Practices.Global Spine J. 2022 Jan;12(1):8-14. doi: 10.1177/2192568220944129. Epub 2020 Aug 5. Global Spine J. 2022. PMID: 32755256 Free PMC article.
-
Reliability and validity of clinical tests to assess the anatomical integrity of the cervical spine in adults with neck pain and its associated disorders: Part 1-A systematic review from the Cervical Assessment and Diagnosis Research Evaluation (CADRE) Collaboration.Eur Spine J. 2017 Sep;26(9):2225-2241. doi: 10.1007/s00586-017-5153-0. Epub 2017 Jun 12. Eur Spine J. 2017. PMID: 28608175
-
Scapular pain in cervical radiculopathy: A scoping review.N Am Spine Soc J. 2025 May 29;23:100619. doi: 10.1016/j.xnsj.2025.100619. eCollection 2025 Sep. N Am Spine Soc J. 2025. PMID: 40620494 Free PMC article. Review.
-
Spurling's test - inconsistencies in clinical practice.J Man Manip Ther. 2021 Feb;29(1):23-32. doi: 10.1080/10669817.2020.1762526. Epub 2020 Jun 30. J Man Manip Ther. 2021. PMID: 32600155 Free PMC article.
-
Clinical characteristics of patients with posterosuperior labral tear: a comparison with patients with other shoulder disorders.J Pain Res. 2018 Sep 10;11:1795-1802. doi: 10.2147/JPR.S166934. eCollection 2018. J Pain Res. 2018. PMID: 30237734 Free PMC article.
References
-
- Ahlgren BD, Gardin SR. Cervical radiculopathy. Orthop Clin North Am. 1996;27:253–263. - PubMed
-
- Bartlett RJ, Hill CR, Gardiner E. A comparison of T2 and gadolinium enhanced MRI with CT myelography in cervical radiculopathy. Br J Radiol. 1998;71:11–19. - PubMed
-
- Bland JH. Clinical methods. In: Bland JH, ed. Disorders of the Cervical Spine. Diagnosis and Medical Management. Philadelphia, PA: WB Saunders; 1987:79–112.
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
