

A novel method for troubleshooting vascular injury during anatomic thoracoscopic pulmonary resection without conversion to thoracotomy
- PMID: 22806532
- PMCID: PMC3580039
- DOI: 10.1007/s00464-012-2475-1
A novel method for troubleshooting vascular injury during anatomic thoracoscopic pulmonary resection without conversion to thoracotomy
Abstract
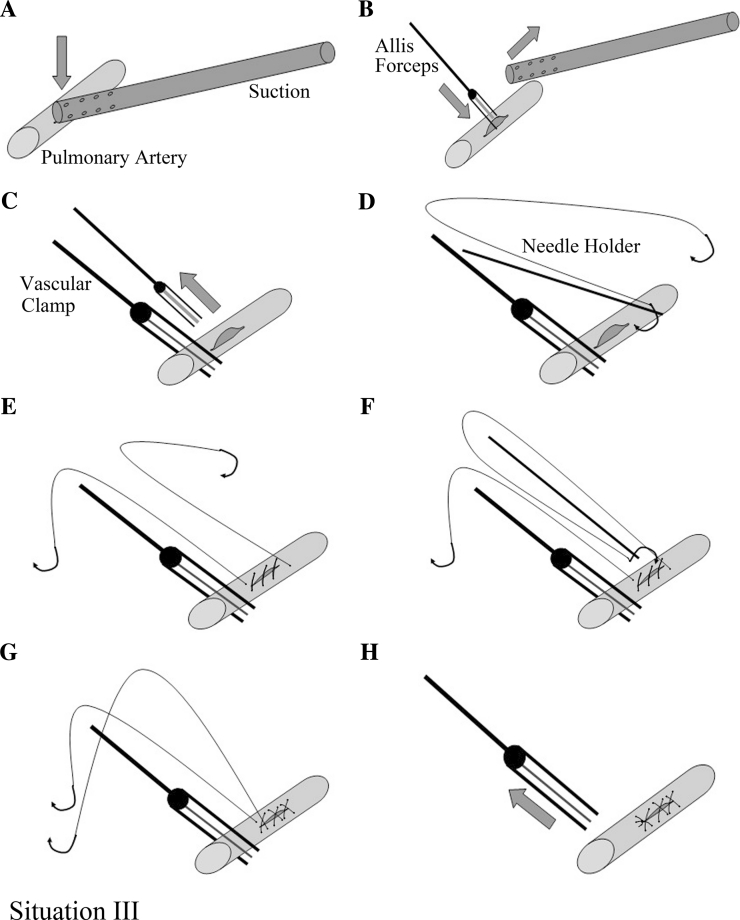
Background: Massive bleeding caused by vascular injury is considered the most troublesome and dangerous complication during video-assisted thoracoscopic surgery (VATS) pulmonary resection and is an important reason for emergency conversion to thoracotomy. The purpose of this paper was to show the suction-compressing angiorrhaphy technique (SCAT) for troubleshooting this problem without conversion.
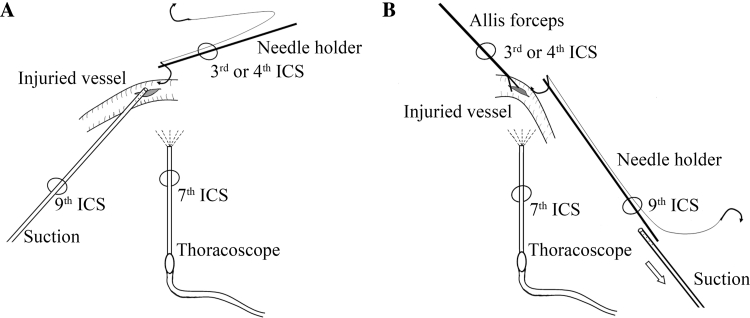
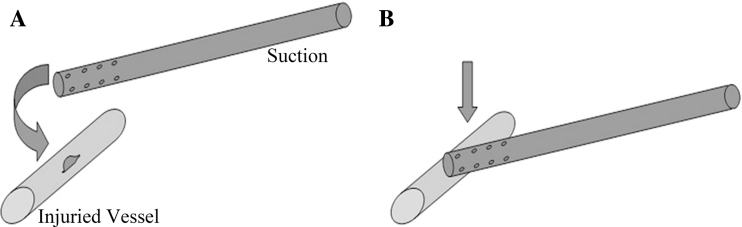
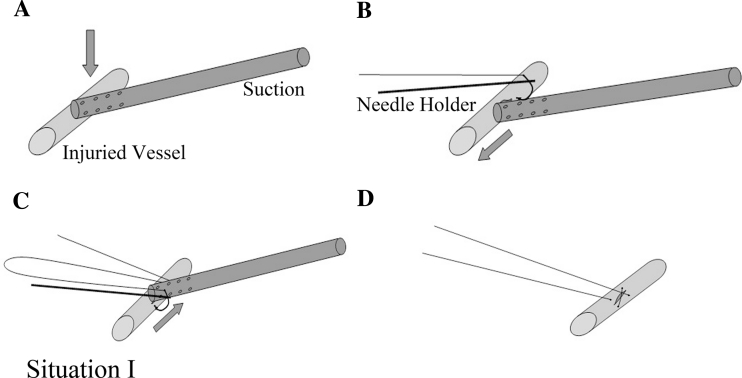
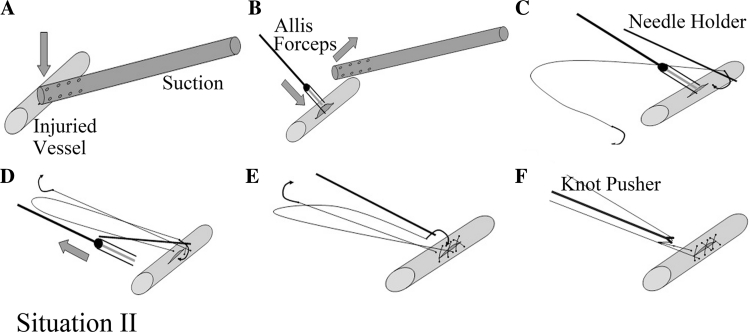
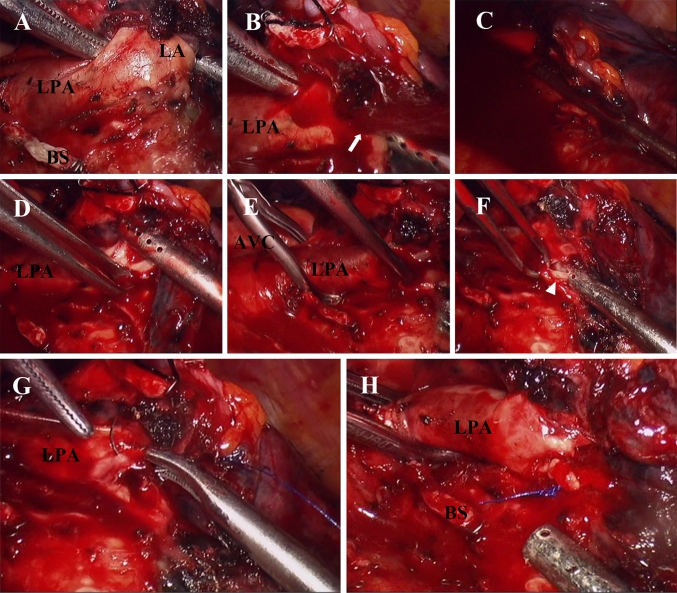
Methods: A total of 414 consecutive VATS anatomic pulmonary resections were performed between May 2006 and July 2011, among which 17 operations (4.11 %) encountered unexpected vascular injury. The procedure for troubleshooting vascular injury included bleeding control and angiorrhaphy. Bleeding was first controlled through side compression of the injured site with an endoscopic suction. Angiorrhaphy was then performed with running 5-0 Prolene suture using different procedures according to the size and location of the injuries, including direct suture upon suction compression, suture after substituting suction compression with clamping of the injured site, or suture after attaining proximal cross-clamping of the main pulmonary artery. Detailed information of these patients was carefully reviewed. The reasons for conversion to thoracotomy also were revealed.
Results: Fifteen cases (15/17, 88.24 %) were successfully managed without conversion. Two cases of left main pulmonary artery injury were converted to thoracotomy due to difficulties in proximal cross-clamping of the injured vessel. Blood loss of the 17 patients ranged from 60-935 (median, 350) ml. Two patients were administered with allogeneic blood. The postoperative chest CT scan showed normal blood flow on the injured vessels. The total conversion rate was 2.66 % (11/414). The most common reason for conversion was hilar lymphadenopathy.
Conclusions: The SCAT is an effective procedure for managing vascular injury during VATS anatomic pulmonary resection. In most cases, bleeding control and angiorrhaphy could be achieved using this method with acceptable blood loss, thereby avoiding emergency conversion to thoracotomy.
Figures
References
-
- Roviaro G, Rebuffat C, Varoli F, Vergani C, Mariani C, Maciocco M. Videoendoscopic pulmonary lobectomy for cancer. Surg Laparosc Endosc. 1992;2:244–247. - PubMed
-
- Whitson BA, Groth SS, Duval SJ, Swanson SJ, Maddaus MA. Surgery for early-stage non-small cell lung cancer: a systematic review of the video-assisted thoracoscopic surgery versus thoracotomy approaches to lobectomy. Ann Thorac Surg. 2008;86:2008–2016. doi: 10.1016/j.athoracsur.2008.07.009. - DOI - PubMed
-
- Yan TD, Black D, Bannon PG, McCaughan BC. Systematic review and meta-analysis of randomized and nonrandomized trials on safety and efficacy of video-assisted thoracic surgery lobectomy for early-stage non-small-cell lung cancer. J Clin Oncol. 2009;27:2553–2562. doi: 10.1200/JCO.2008.18.2733. - DOI - PubMed
-
- Ettinger DS, Akerley W, Bepler G, Blum MG, Chang A, Cheney RT, Chirieac LR, D’Amico TA, Demmy TL, Ganti AKP, Govindan R, Grannis FW, Jr, Jahan T, Jahanzeb M, Johnson DH, Kessinger A, Komaki R, Kong F-M, Kris MG, Krug LM, Le Q-T, Lennes IT, Martins R, O’Malley J, Osarogiagbon RU, Otterson GA, Patel JD, Pisters KM, Reckamp K, Riely GJ, Rohren E, Simon GR, Swanson SJ, Wood DE, Yang SC, Members NN-SCLCP, Riely G. Non-small cell lung cancer. J Natl Compr Cancer Netw. 2010;8:740–801. - PubMed
-
- Maehara T, Takei H, Nishii T, Itoh H, Inui K, Watanabe K, Nakayama H. Intraoperative conversion and postoperative complication of video-assisted thoracoscopic surgery lobectomy for primary lung cancer. Kyobu Geka. 2003;56:939–942. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
