

Battlefield radiology
- PMID: 22806621
- PMCID: PMC3611714
- DOI: 10.1259/bjr/33335273
Battlefield radiology
Abstract
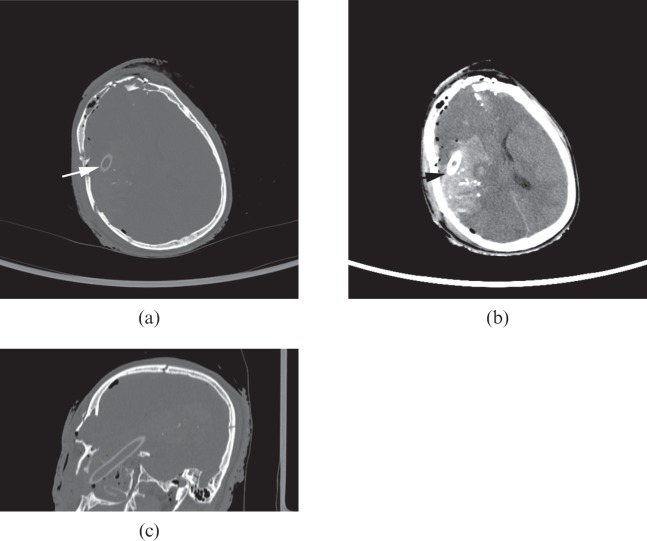
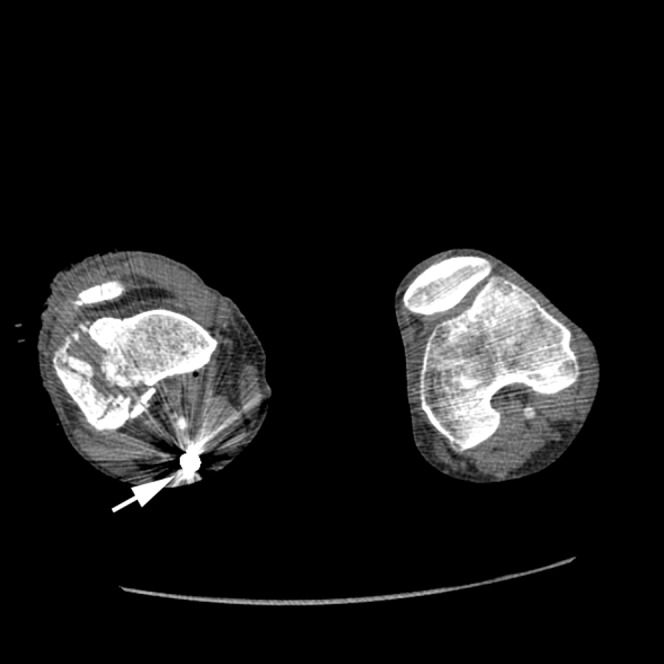
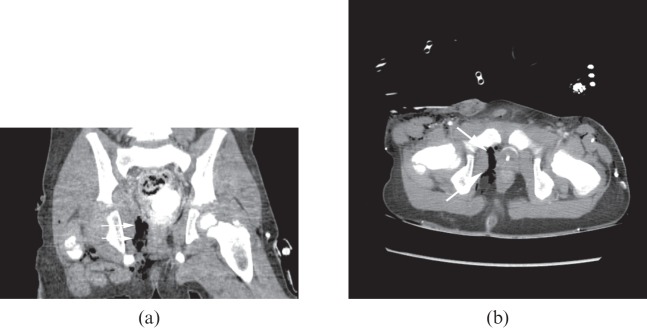
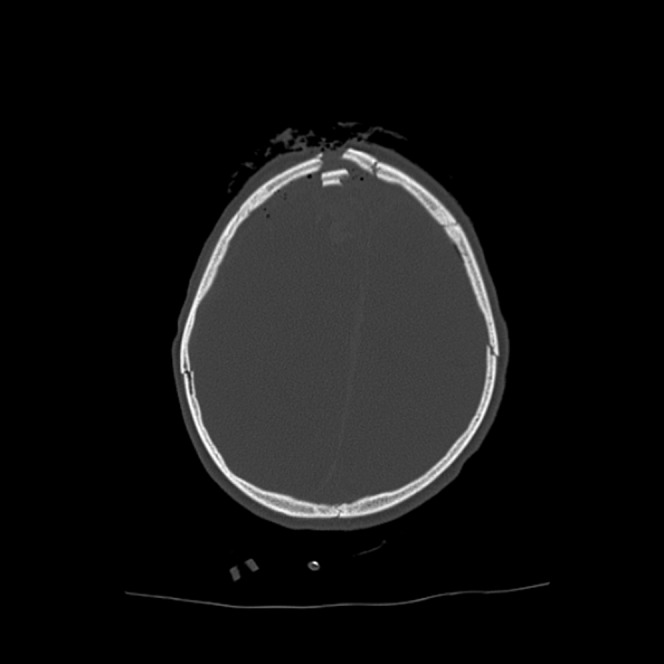
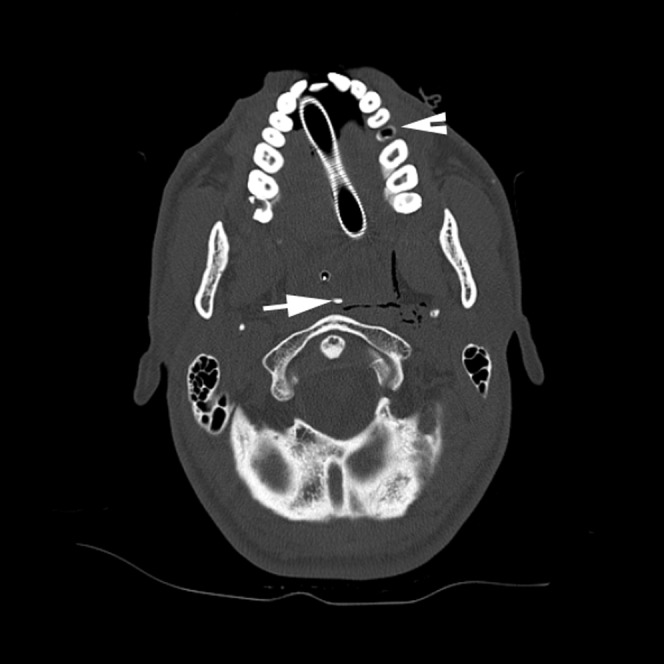
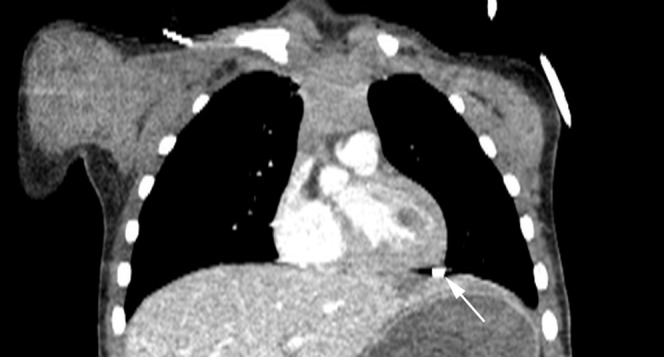
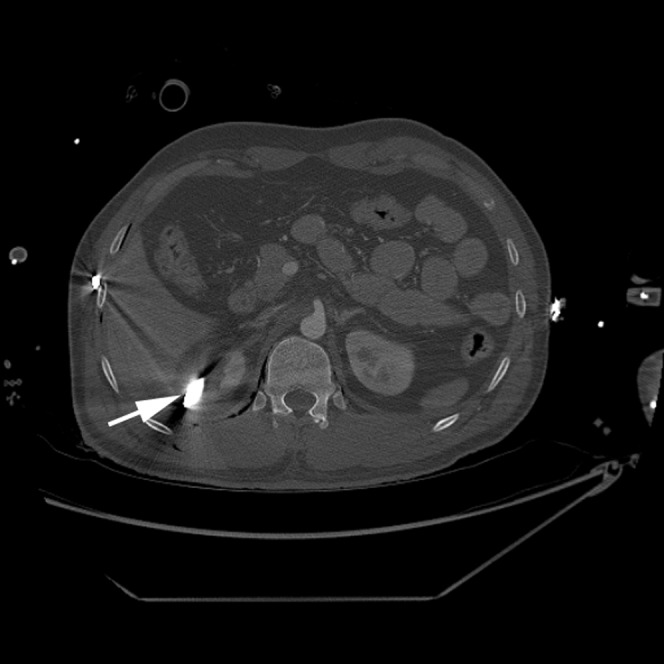
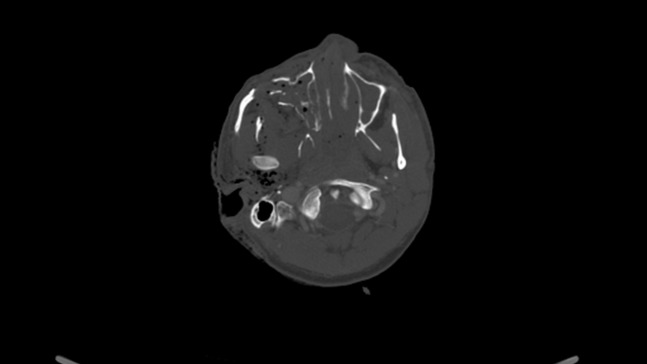
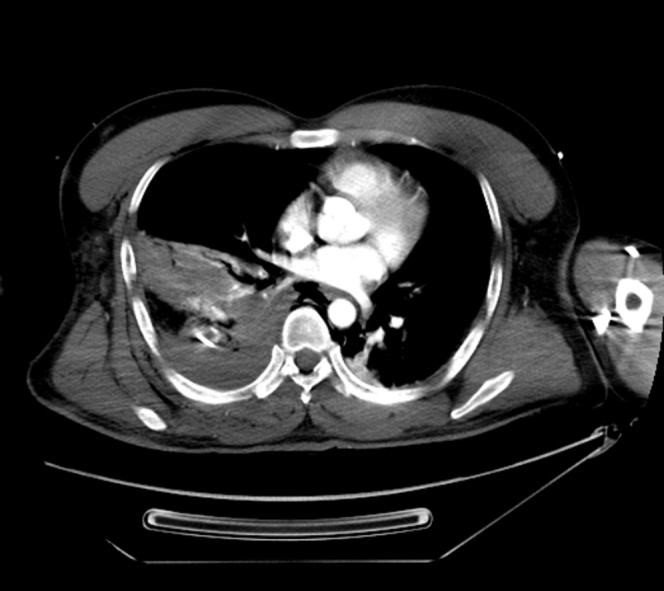
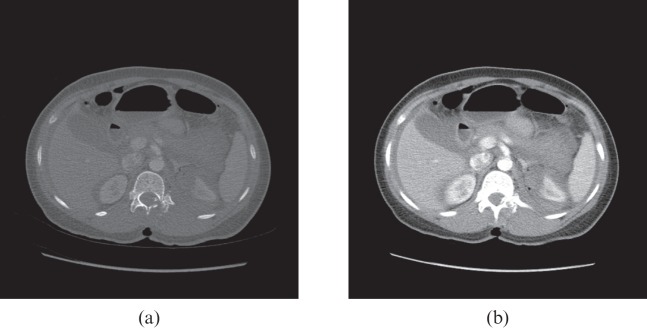
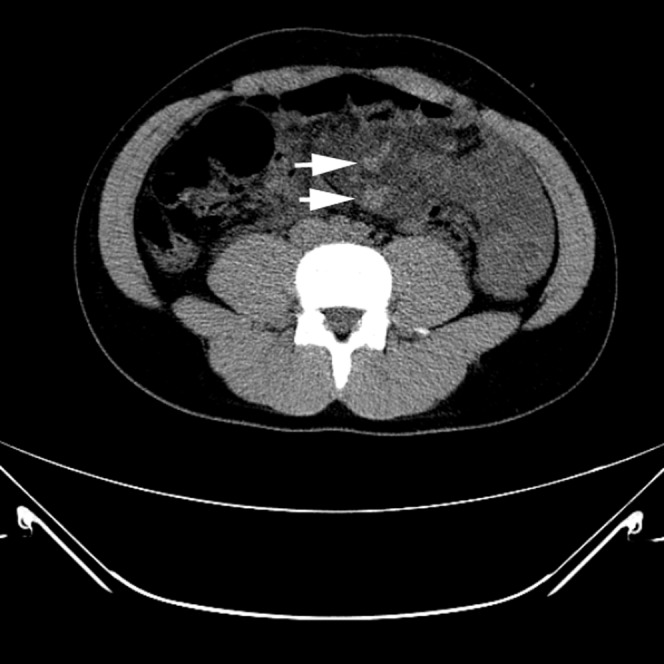
With the increasing tempo of military conflicts in the last decade, much has been learnt about imaging battlefield casualties in the acute setting. Ultrasound in the form of focused abdominal sonography in trauma (FAST) has proven invaluable in emergency triage of patients for immediate surgery. Multidetector CT allows accurate determination of battlefield trauma injuries. It permits the surgeons and anaesthetists to plan their interventions more thoroughly and to be made aware of clinically occult injuries. There are common injury patterns associated with blast injury, gunshot wounds and blunt trauma. While this body of knowledge is most applicable to the battlefield, there are parallels with peacetime radiology, particularly in terrorist attacks and industrial accidents. This pictorial review is based on the experiences of a UK radiologist deployed in Afghanistan in 2010.
Figures







Similar articles
-
Understanding the burden of injury in children from conflict: an analysis of radiological imaging from a Role 3 hospital in Afghanistan in 2011.BMJ Mil Health. 2024 Dec 11;170(e2):e116-e121. doi: 10.1136/military-2022-002336. BMJ Mil Health. 2024. PMID: 37045540
-
"Einsatzchirurgie"--experiences of German military surgeons in Afghanistan.Langenbecks Arch Surg. 2011 Apr;396(4):507-22. doi: 10.1007/s00423-011-0760-4. Epub 2011 Mar 8. Langenbecks Arch Surg. 2011. PMID: 21384192 Review.
-
FAST in the deployed military setting.J R Army Med Corps. 2018 Sep;164(5):332-334. doi: 10.1136/jramc-2018-000906. Epub 2018 Apr 10. J R Army Med Corps. 2018. PMID: 29643121
-
The burden of gunshot wounding of UK military personnel in Iraq and Afghanistan from 2003-14.Injury. 2018 Jun;49(6):1064-1069. doi: 10.1016/j.injury.2018.03.028. Epub 2018 Mar 27. Injury. 2018. PMID: 29609973
-
[Acute abdominal trauma].Radiologe. 2019 Feb;59(2):139-145. doi: 10.1007/s00117-018-0485-2. Radiologe. 2019. PMID: 30627752 Review. German.
Cited by
-
Comparison of image quality of split-bolus computed tomography versus dual-phase computed tomography in abdominal trauma.Pol J Radiol. 2025 Mar 31;90:e151-e160. doi: 10.5114/pjr/200756. eCollection 2025. Pol J Radiol. 2025. PMID: 40321708 Free PMC article.
-
Combat radiology: Challenges and opportunities.Med J Armed Forces India. 2017 Oct;73(4):410-413. doi: 10.1016/j.mjafi.2017.09.014. Epub 2017 Nov 15. Med J Armed Forces India. 2017. PMID: 29386721 Free PMC article.
-
Trauma whole-body MDCT: an assessment of image quality in conventional dual-phase and modified biphasic injection.Br J Radiol. 2016 Jul;89(1063):20160160. doi: 10.1259/bjr.20160160. Epub 2016 May 17. Br J Radiol. 2016. PMID: 27187601 Free PMC article.
-
Bowel and mesenteric injuries in blunt abdominal injury.Singapore Med J. 2024 Jun 1;65(6):354-359. doi: 10.4103/singaporemedj.SMJ-2022-023. Epub 2024 Jun 4. Singapore Med J. 2024. PMID: 38834940 Free PMC article. No abstract available.
-
Pearls and pitfalls in imaging of blunt traumatic thoracic aortic injury: a pictorial review.Br J Radiol. 2018 Sep;91(1089):20180130. doi: 10.1259/bjr.20180130. Epub 2018 Apr 16. Br J Radiol. 2018. PMID: 29644869 Free PMC article. Review.
References
-
- Ramoutsaki IA, Giannacos EN, Livadas GN. Birth of battlefield radiology: Greco-Turkish War of 1897. Radiographics 2001;21:263–6 - PubMed
-
- Patel NY, Riherd JM. Focused assessment with sonography for trauma: methods, accuracy, and indications. Surg Clin North Am 2011;91:195–207 - PubMed
-
- Holcomb JB, Helling TS, Hirshberg A. Military, civilian, and rural application of the damage control philosophy. Mil Med 2001;166:490–3 - PubMed
-
- Nguyen D, Platon A, Shanmuganathan K, Mirvis SE, Becker CD, Poletti PA. Evaluation of a single-pass continuous whole-body 16-MDCT protocol for patients with polytrauma. AJR Am J Roentgenol 2009;192:3–10 - PubMed
-
- Ramasamy A, Harrisson SE, Clasper JC, Stewart MP. Injuries from roadside improvised explosive devices. J Trauma 2008;65:910–14 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
