

Non-clear cell renal cell carcinoma: does the mammalian target of rapamycin represent a rational therapeutic target?
- PMID: 22807514
- PMCID: PMC3425523
- DOI: 10.1634/theoncologist.2012-0038
Non-clear cell renal cell carcinoma: does the mammalian target of rapamycin represent a rational therapeutic target?
Abstract
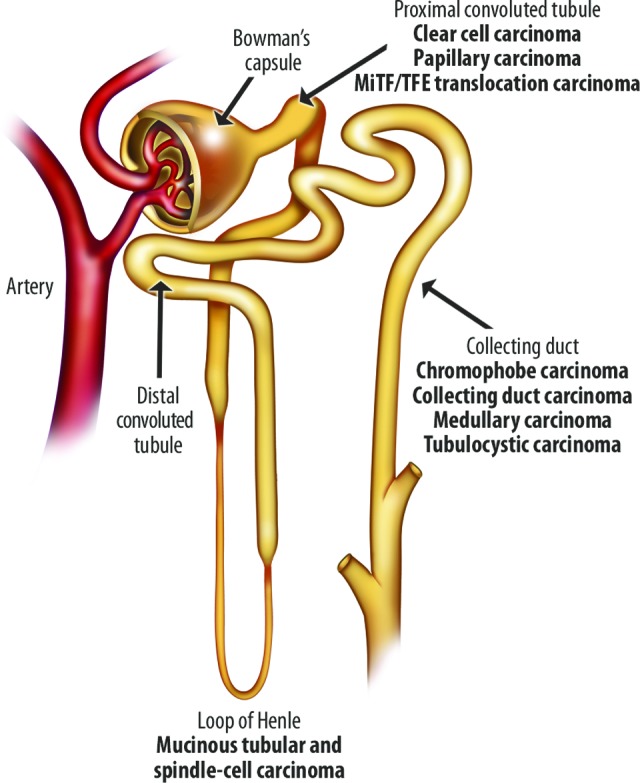
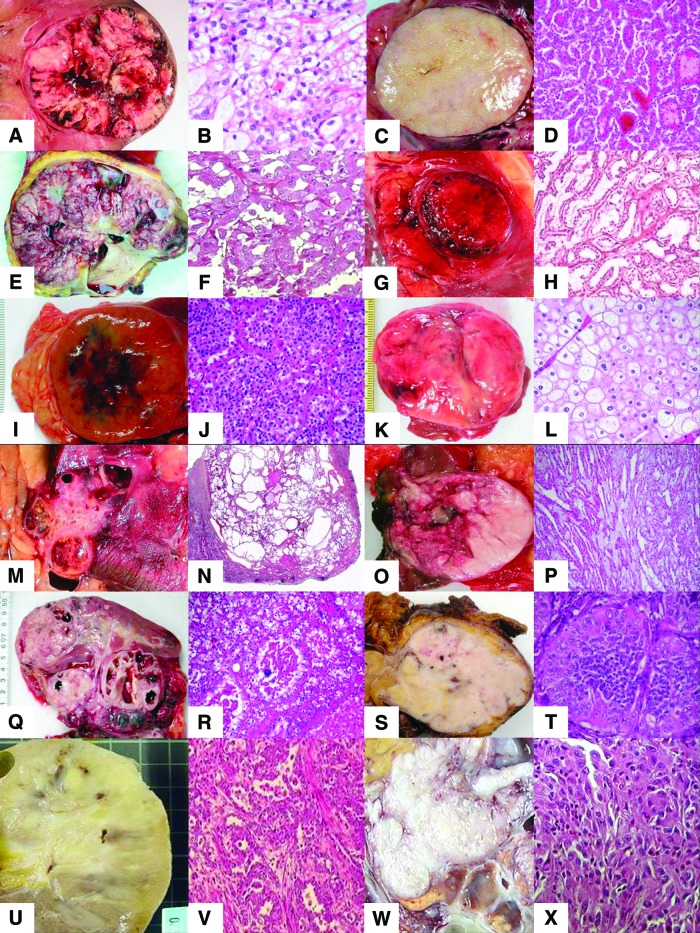
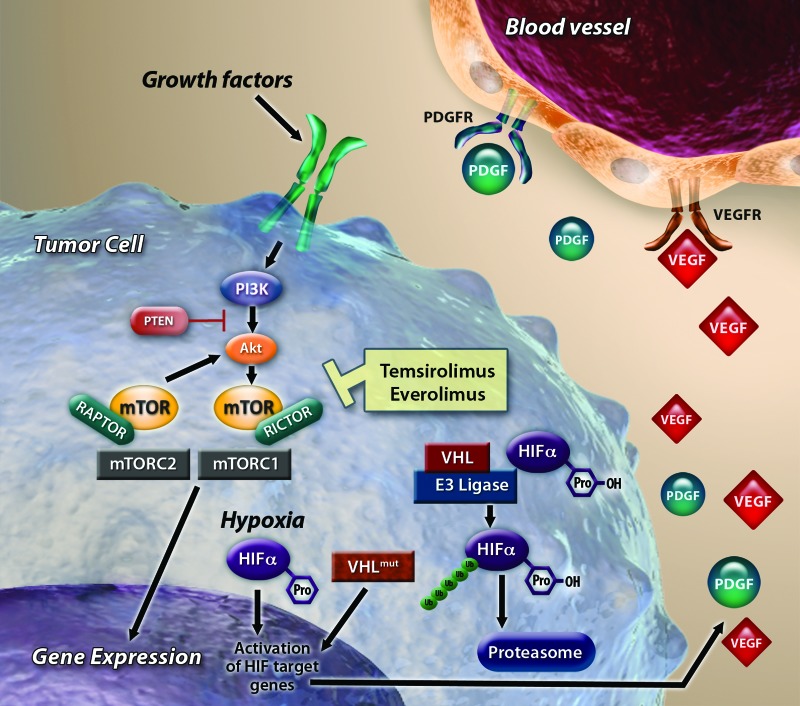
Non-clear cell renal cell carcinomas (nccRCCs) comprise a heterogenous and poorly characterized group of tumor types for which few treatments have been approved. Although targeted therapies have become the cornerstones of systemic treatment for metastatic renal cell carcinoma, patients with nccRCC have been excluded from many pivotal clinical trials. As such, robust clinical evidence supporting the use of these agents in patients with nccRCC is lacking. Here, we review the disparate nccRCC subtypes, the criteria for diagnosis, and the prognoses associated with each subtype, in addition to evaluating the potential use of mammalian target of rapamycin (mTOR) inhibitors in treating patients with nccRCC. Both genetic analyses and preclinical research indicate a central role for mTOR in nccRCC; a therapy that targets this ubiquitous regulator of cellular signaling could prove efficacious across various tumor subtypes. Results from recent studies exploring targeted therapies as both monotherapy and combination therapy have provided early indications of efficacy in patients with nccRCC. Exploratory analyses support further research with the mTOR inhibitors everolimus and temsirolimus in patients with nccRCC. Current clinical practice guidelines support the use of mTOR inhibitors in patients with nccRCC; however, these recommendations are based on low levels of evidence. Further results from randomized, controlled clinical trials are needed to determine the optimal choice of therapy for patients with nccRCC. Results from ongoing clinical trials of mTOR inhibitors and other agents in nccRCC, as well as their impact on the nccRCC treatment paradigm, are eagerly awaited.
Conflict of interest statement
Figures

Similar articles
-
Targeted therapies and the treatment of non-clear cell renal cell carcinoma.Ann Oncol. 2013 Jul;24(7):1730-1740. doi: 10.1093/annonc/mdt152. Epub 2013 Apr 26. Ann Oncol. 2013. PMID: 23625974 Review.
-
Future directions of mammalian target of rapamycin (mTOR) inhibitor therapy in renal cell carcinoma.Target Oncol. 2011 Mar;6(1):5-16. doi: 10.1007/s11523-011-0172-y. Epub 2011 Apr 12. Target Oncol. 2011. PMID: 21484496 Free PMC article. Review.
-
Rechallenge with mTOR inhibitors in metastatic renal cell carcinoma patients who progressed on previous mTOR inhibitor therapy.Oncology. 2013;85(1):8-13. doi: 10.1159/000350005. Epub 2013 Jun 21. Oncology. 2013. PMID: 23797151
-
Oral and intravenously administered mTOR inhibitors for metastatic renal cell carcinoma: pharmacokinetic considerations and clinical implications.Cancer Treat Rev. 2013 Nov;39(7):784-92. doi: 10.1016/j.ctrv.2012.12.012. Epub 2013 Jan 30. Cancer Treat Rev. 2013. PMID: 23375248 Review.
-
Everolimus in the treatment of renal cell carcinoma and neuroendocrine tumors.Adv Ther. 2010 Aug;27(8):495-511. doi: 10.1007/s12325-010-0045-2. Epub 2010 Jul 8. Adv Ther. 2010. PMID: 20623346 Review.
Cited by
-
Optimal management of metastatic renal cell carcinoma: current status.Drugs. 2013 Apr;73(5):427-38. doi: 10.1007/s40265-013-0043-1. Drugs. 2013. PMID: 23572408 Review.
-
Renal cell carcinoma: new insights and challenges for a clinician scientist.Am J Physiol Renal Physiol. 2017 Aug 1;313(2):F145-F154. doi: 10.1152/ajprenal.00480.2016. Epub 2017 Apr 5. Am J Physiol Renal Physiol. 2017. PMID: 28381462 Free PMC article. Review.
-
The efficacy of molecular targeted therapy and nivolumab therapy for metastatic non-clear cell renal cell carcinoma: A retrospective analysis using the Michinoku Japan urological cancer study group database.Cancer Med. 2023 Nov;12(22):20677-20689. doi: 10.1002/cam4.6591. Epub 2023 Oct 31. Cancer Med. 2023. PMID: 37905674 Free PMC article.
-
Everolimus Versus Sunitinib Prospective Evaluation in Metastatic Non-Clear Cell Renal Cell Carcinoma (ESPN): A Randomized Multicenter Phase 2 Trial.Eur Urol. 2016 May;69(5):866-74. doi: 10.1016/j.eururo.2015.10.049. Epub 2015 Nov 26. Eur Urol. 2016. PMID: 26626617 Free PMC article. Clinical Trial.
References
-
- National Cancer Institute. SEER stat fact sheets: Kidney and renal pelvis. [Accessed June 11, 2010]. Available at http://seer.cancer.gov/statfacts/html/kidrp.html.
-
- Ferlay J, Parkin DM, Steliarova-Foucher E. Estimates of cancer incidence and mortality in Europe in 2008. Eur J Cancer. 2010;46:765–781. - PubMed
-
- Cohen HT, McGovern FJ. Renal-cell carcinoma. N Engl J Med. 2005;353:2477–2490. - PubMed
-
- Latif F, Mubarak M, Kazi JI. Histopathological characteristics of adult renal tumours: A preliminary report. J Pak Med Assoc. 2011;61:224–228. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
