

Chronic hepatitis C treatment outcomes in low- and middle-income countries: a systematic review and meta-analysis
- PMID: 22807600
- PMCID: PMC3397704
- DOI: 10.2471/BLT.11.097147
Chronic hepatitis C treatment outcomes in low- and middle-income countries: a systematic review and meta-analysis
Abstract
Objective: To assess the effectiveness of treatment for hepatitis C virus (HCV) infection in low- and middle-income countries and identify factors associated with successful outcomes.
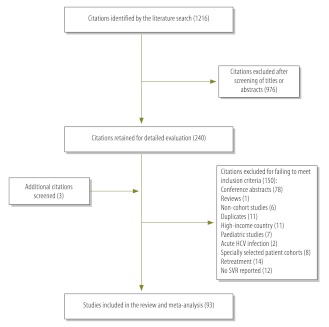
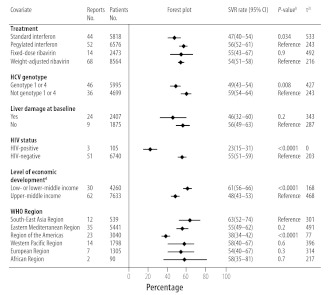
Methods: We performed a systematic review and meta-analysis of studies of HCV treatment programmes in low- and middle-income countries. The primary outcome was a sustained virological response (SVR). Factors associated with treatment outcomes were identified by random-effects meta-regression analysis.
Findings: The analysis involved data on 12 213 patients included in 93 studies from 17 countries. The overall SVR rate was 52% (95% confidence interval, CI: 48-56). For studies in which patients were predominantly infected with genotype 1 or 4 HCV, the pooled SVR rate was 49% (95% CI: 43-55). This was significantly lower than the rate of 59% (95% CI: 54-64) found in studies in which patients were predominantly infected with other genotypes (P = 0.012). Factors associated with successful outcomes included treatment with pegylated interferon and ribavirin, infection with an HCV genotype other than genotype 1 or 4 and the absence of liver damage or human immunodeficiency virus infection at baseline. No significant difference in the SVR rate was observed between weight-adjusted and fixed-dose ribavirin treatment. Overall, 17% (95% CI: 13-23) of adverse events resulted in treatment interruption or dose modification, but only 4% (95% CI: 3-5) resulted in treatment discontinuation.
Conclusion: The outcomes of treatment for HCV infection in low- and middle-income countries were similar to those reported in high-income countries.
Objectif: Évaluer l’efficacité du traitement de l’infection par le virus de l’hépatite C (VHC) dans les pays à revenu faible et moyen et identifier les facteurs associés aux résultats positifs.
Méthodes: Nous avons effectué une évaluation systématique et une méta-analyse des études sur les programmes de traitement du VHC dans les pays à revenu faible et moyen. Le résultat principal consistait en une réponse virologique soutenue (RVS). Les facteurs liés aux résultats du traitement ont été identifiés à l'aide d'une analyse de méta-régression des effets aléatoires.
Résultats: L'analyse portait sur les données de 12 213 patients inclus dans 93 études provenant de 17 pays différents. Le taux de RVS général était de 52% (intervalle de confiance de 95%, IC: 48-56). Pour les études dans lesquelles les patients étaient principalement atteints par le VHC de génotype 1 ou 4, le taux de RVS groupé était de 49% (IC de 95%: 43-55). Ce taux était largement inférieur à celui de 59% (IC de 95%: 54-64) présenté dans les études dans lesquelles les patients étaient principalement atteints par d'autres génotypes (P = 0,012). Les facteurs liés aux résultats positifs incluaient le traitement à l'interféron pégylé et à la ribavirine, l'infection à un VHC de génotype autre que 1 ou 4 et l'absence de lésions au foie ou d'infection par le virus de l'immunodéficience humaine initialement. Aucune différence significative dans le taux de RVS n'a été observée entre les traitements de ribavirine adaptés au poids et ceux à dose fixe. Dans l'ensemble, 17% (IC de 95%: 13-23) des effets indésirables ont entraîné une interruption du traitement ou une modification des doses, tandis que 4% (IC de 95%: 3-5) d'entre eux ont entraîné un abandon du traitement.
Conclusion: Les résultats du traitement de l’infection du VHC dans les pays à revenu faible et moyen étaient similaires à ceux qui étaient indiqués dans les pays à revenu élevé.
Objetivo: Determinar la efectividad del tratamiento para la infección por el virus de la hepatitis C (VHC) en países de ingresos medios y bajos e identificar los factores asociados con unos resultados satisfactorios.
Métodos: Realizamos un examen sistemático y un meta-análisis de estudios de programas de tratamiento del VHC en países de ingresos medios y bajos. El resultado fundamental fue una respuesta viral sostenida (RVS). Los factores asociados con los resultados del tratamiento se identificaron mediante un análisis de metarregresión de efectos aleatorios.
Resultados: El análisis incluyó datos sobre 12 213 pacientes en 93 estudios de 17 países. La tasa global de RVS fue del 52% (intervalo de confianza, IC del 95%: 48–56). Para estudios en los que los pacientes estaban predominantemente infectados con VHC del genotipo 1 o 4, la tasa de RVS combinada fue del 49% (IC del 95%: 43–55). Esta fue significativamente menor que la tasa del 59% (IC del 95%: 54–64) encontrada en estudios en los que los pacientes estaban predominantemente infectados con otros genotipos (P = 0,012). Los factores asociados con los resultados satisfactorios incluyeron el tratamiento con interferón pegilado y ribavirina, la infección del VHC de un genotipo distinto al 1 o al 4 y la ausencia de lesión hepática o de infección por el virus de la inmunodeficiencia humana en el inicio. No se observaron diferencias significativas en la tasa de RVS entre el tratamiento de ribavirina adaptado al peso del paciente y el de dosis fijas. En conjunto, el 17% (IC del 95%: 13–23) de los eventos adversos provocó la interrupción del tratamiento o la modificación de la dosis, mientras que el 4% (IC del 95%: 3–5) causó el abandono del tratamiento.
Conclusión: Los resultados del tratamiento de la infección del VHC en países de ingresos bajos y medios fueron similares a los de países de ingresos elevados.
الغرض: تقييم فعالية علاج عدوى فيروس التهاب الكبد C (HCV) في البلدان منخفضة ومتوسطة الدخل وتحديد العوامل المرتبطة بالنتائج الناجحة.
الطريقة: أجرينا استعراضاً منهجياً وتحليلاً وصفياً لدراسات برامج علاج فيروس التهاب الكبد C في البلدان منخفضة ومتوسطة الدخل. وكانت النتيجة الأولية استجابة فيروسية مستديمة (SVR). وتم تحديد العوامل المرتبطة بنتائج العلاج من خلال تحليل الارتداد الوصفي للآثار العشوائية.
النتائج:
اشتمل التحليل على بيانات حول 12213 مريضًا تم إدراجهم في 93 دراسة من 17 بلدًا. وكان المعدل الكلي للاستجابة الفيروسية المستديمة 52
الاستنتاج: كانت نتائج علاج عدوى فيروس التهاب الكبد C في البلدان منخفضة ومتوسطة الدخل متشابهة مع تلك المبلغ عنها في البلدان مرتفعة الدخل.
目的: 评估中低收入国家治疗丙型肝炎病毒(HCV)感染的效果并确定成功结果的相关因素。
方法: 我们对中低收入国家的丙型肝炎病毒治疗方案研究进行了系统性回顾和元分析。主要成果是治疗持续病毒学响应(SVR)。随机效应元回归分析确定与治疗效果相关的因素。
结果: 分析来自17 个国家93 个研究中涉及12213 例病患的数据。总体SVR率为52%(95%置信区间,CI:48-56)。对于患者主要感染基因型1 或4 丙型肝炎病毒的研究,合并的SVR率为49%(95% CI:43-55);在患者主要感染其他基因型病毒(p =0.012)的研究中发现的SVR率为59%(95% CI:54-64),前者比率显著低于后者。与成功结果关联的因素包括使用聚乙二醇干扰素和利巴韦林治疗、感染非基因型1 或4 的基因型丙型肝炎病毒、无肝损害或者基线艾滋病毒感染。在权重调整和固定剂量的利巴韦林治疗之间未观察到SVR率的显著差异。总体而言,17%(95% CI:13-23)的不良事件导致治疗间断或剂量调整,而 4%(95% CI:3-5)的不良事件导致治疗终止。
结论: 中低收入国家丙型肝炎病毒感染治疗的效果与高收入国家报道的效果相似。
Цель: Оценить эффективность лечения вируса гепатита С (ВГС) в странах с низким и средним уровнем дохода, а также определить факторы, влияющие на достижение успешных результатов.
Методы: Мы провели систематический обзор и мета-анализ исследований, посвященных программам лечения ВГC в странах с низким и средним уровнем дохода. В качестве основного параметра оценки было выбранополучение устойчивого вирусологического ответа (УВО). Факторы, связанные с результатами лечения, идентифицировались с помощью мета-регрессионного анализа на основе модели случайных эффектов.
Результаты: Были проанализированы данные о 12 213 пациентах, участвовавших в 93 исследованиях в 17 странах. Общий уровень УВО составил 52% (доверительный интервал, ДИ 95%: 48–56). Для исследований, в которых пациенты были инфицированы преимущественно ВГС с генотипом 1 или 4, агрегированное значение УВО составило 49% (ДИ 95%: 43–55). Это было значительно ниже уровня 59% (ДИ 95%: 54–64), выявленного в исследованиях, в которых пациенты были инфицированы преимущественно другими генотипами (P = 0,012). Факторы, влияющие на достижение успешных результатов, включали лечение пегилированным интерфероном и рибавирином, инфицирование генотипом, отличным от 1 и 4, а также отсутствие повреждения печени или вируса иммунодефицита человека на начальном этапе. Не наблюдалось каких-либо существенных различий в уровне УВО между дозировкой рибавирина в зависимости от массы тела и фиксированной дозировкой. В целом, 17% (ДИ 95%: 13–23) нежелательных реакций приводили к прерыванию лечения или изменению дозировки, а 4% (ДИ 95%: 3–5) – к прекращению лечения.
Вывод: Результаты лечения инфекции ВГС в странах с низким и средним уровнем дохода были схожи с теми, о которых отчитываются в странах с высоким уровнем доходов.
Figures
References
-
- Viral hepatitis: global policy London: World Hepatitis Alliance; 2011. Available from: http://www.worldhepatitisalliance.org/Policy/2010PolicyReport.aspxhttp://[accessed 12 January 2012].
-
- Viral hepatitis. WHA63.18. Sixty-third World Health Assembly. Agenda item 11.12. Geneva: World Health Organization; 2010. Available from: http://apps.who.int/gb/ebwha/pdf_files/WHA63/A63_R18-en.pdfhttp://[accessed 12 January 2012].
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources