

Efficacy of hepatic arterial infusion chemotherapy in advanced hepatocellular carcinoma
- PMID: 22807613
- PMCID: PMC3396196
- DOI: 10.3748/wjg.v18.i26.3426
Efficacy of hepatic arterial infusion chemotherapy in advanced hepatocellular carcinoma
Abstract
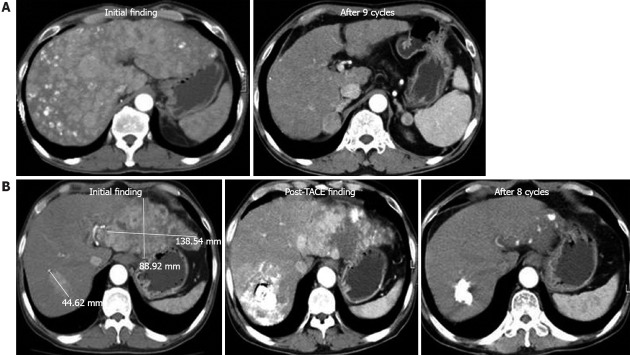
Aim: To investigate the efficacy of hepatic arterial infusion chemotherapy (HAIC) using floxuridine (FUDR) in patients with advanced hepatocellular carcinoma (HCC) confined to the liver.
Methods: Thirty-four patients who had advanced HCC with unresectability or unsuccessful previous therapy in the absence of extrahepatic metastasis were treated with intra-arterial FUDR chemotherapy at our hospital between March 2005 and May 2008. Among the 34 patients, 9 patients were classified as Child class C, and 18 patients had portal vein tumor thrombus (PVTT). One course of chemotherapy consisted of continuous infusion of FUDR (0.3 mg/kg during day 1-14) and dexamethasone (10 mg on day 1, 4, 7 and 11), and this treatment was repeated every 28 d.
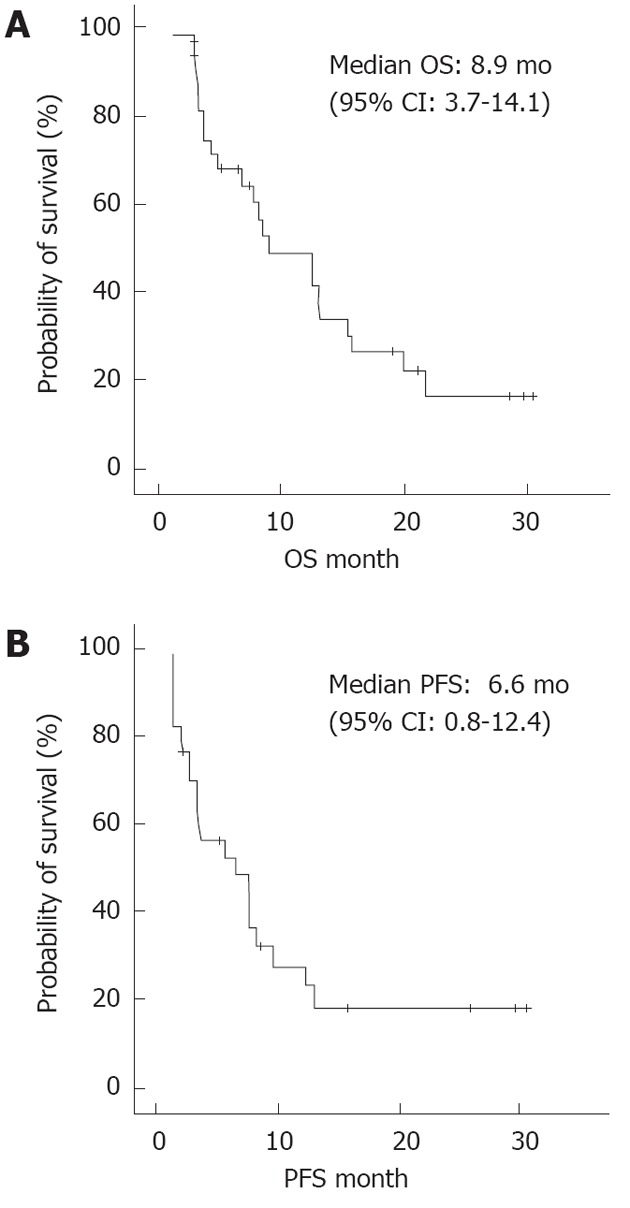
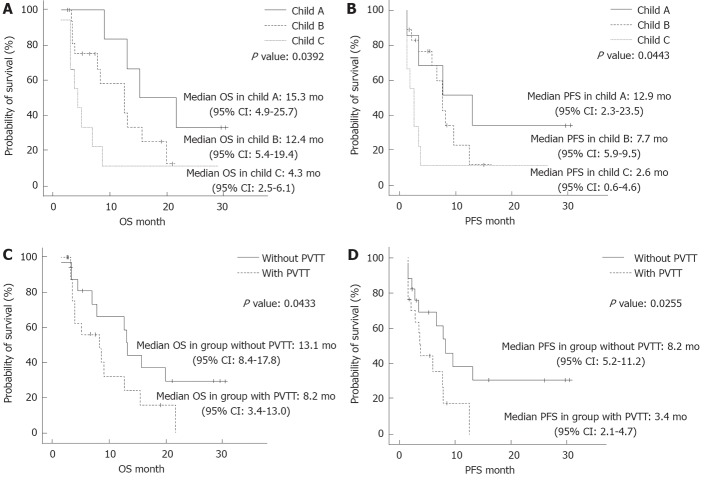
Results: Two patients (5.9%) displayed a complete response, and 12 patients (35.3%) had a partial response. The tumor control rate was 61.8%. The median overall survival times were 15.3 mo, 12.4 mo and 4.3 mo for the patients who were classified as Child class A, Child class B and Child class C, respectively (P = 0.0392). The progression-free survival was 12.9 mo, 7.7 mo and 2.6 mo for the patients who were classified as Child class A, Child class B and Child class C, respectively (P = 0.0443). The cumulative survival differed significantly according to the Child-Pugh classification and the presence of PVTT. In addition to hepatic reserve capacity and PVTT, the extent of HCC was an independent factor in determining a poor prognosis. The most common adverse reactions to HAIC were mucositis, diarrhea and peptic ulcer disease, but most of these complications were improved by medical treatment and/or a delay of HAIC.
Conclusion: The present study demonstrates that intra-arterial FUDR chemotherapy is a safe and effective treatment for advanced HCC that is recalcitrant to other therapeutic modalities, even in patients with advanced cirrhosis.
Keywords: Advanced hepatocellular carcinoma; Child-Pugh classification; Floxuridine; Hepatic arterial infusion chemotherapy; Portal vein tumor thrombus.
Figures
References
-
- Parkin DM, Bray F, Ferlay J, Pisani P. Estimating the world cancer burden: Globocan 2000. Int J Cancer. 2001;94:153–156. - PubMed
-
- Lee JS. Advances in the treatment of hepatocellular carcinoma. Korean J Med. 2009;77:290–297.
-
- Makuuchi M, Hasegawa H, Yamazaki S. Ultrasonically guided subsegmentectomy. Surg Gynecol Obstet. 1985;161:346–350. - PubMed
-
- Ohtomo K, Furui S, Kokubo T, Yamauchi T, Itai Y, Yashiro N, Iio M. Transcatheter arterial embolization (TAE) in treatment for hepatoma--analysis of three-year survivors. Radiat Med. 1985;3:176–180. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
