

Endoscopic therapy for gastric stromal tumors originating from the muscularis propria
- PMID: 22807618
- PMCID: PMC3396201
- DOI: 10.3748/wjg.v18.i26.3465
Endoscopic therapy for gastric stromal tumors originating from the muscularis propria
Abstract
Aim: To explore endoscopic therapy methods for gastric stromal tumors originating from the muscularis propria.
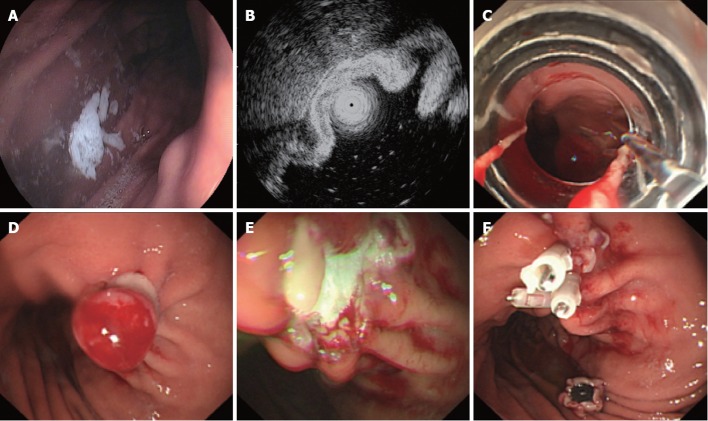
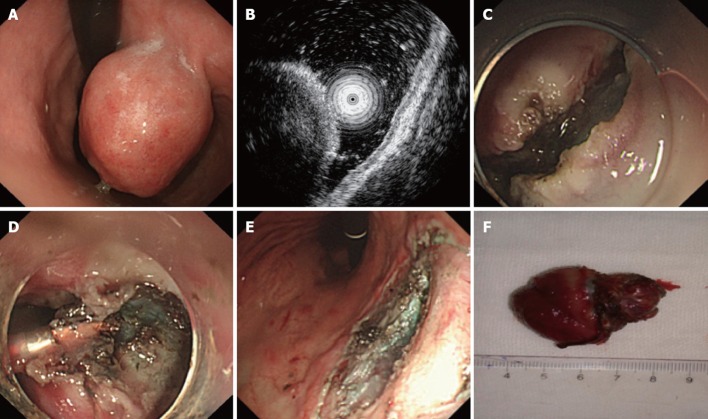
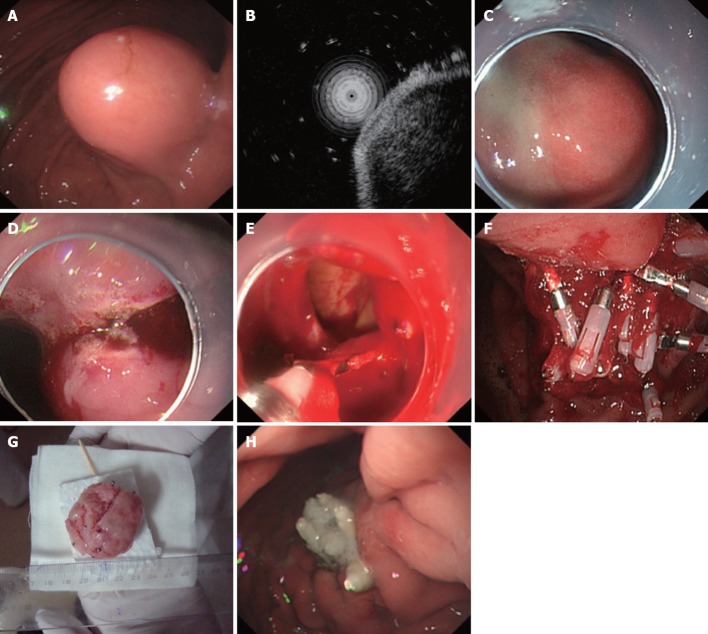
Methods: For 69 cases diagnosed as gastric stromal tumors originating from the muscularis propria, three types of endoscopic therapy were selected, based on the size of the tumor. These methods included endoscopic ligation and resection (ELR), endoscopic submucosal excavation (ESE) and endoscopic full-thickness resection (EFR). The wound surface and the perforation of the gastric wall were closed with metal clips. Immunohistostaining for CD34, CD117, Dog-1, S-100 and smooth muscle actin (SMA) was performed on the resected tumors.
Results: A total of 38 cases in which the tumor size was less than 1.2 cm were treated with ELR; three cases were complicated by perforation, and the perforations were closed with metal clips. Additionally, 18 cases in which the tumor size was more than 1.5 cm were treated with ESE, and no perforation occurred. Finally, 13 cases in which the tumor size was more than 2.0 cm were treated with EFR; all of the cases were complicated by artificial perforation, and all of the perforations were closed with metal clips. All of the 69 cases recovered with medical treatment, and none required surgical operation. Immunohistostaining demonstrated that among all of the 69 gastric stromal tumors diagnosed by gastroscopy, 12 cases were gastric leiomyomas (SMA-positive), and the other 57 cases were gastric stromal tumors.
Conclusion: Gastric stromal tumors originating from the muscularis propria can be treated successfully with endoscopic techniques, which could replace certain surgical operations and should be considered for further application.
Keywords: Endoscopy; Gastrointestinal stromal tumors; Muscularis propria; Resection; Therapy.
Figures
References
-
- Orsenigo E, Gazzetta P, Palo SD, Tamburini A, Staudacher C. Experience on surgical treatment of gastrointestinal stromal tumor of the stomach. Updates Surg. 2010;62:101–104. - PubMed
-
- Tanabe K, Urabe Y, Tokumoto N, Suzuki T, Yamamoto H, Oka S, Tanaka S, Ohdan H. A new method for intraluminal gastrointestinal stromal tumor resection using laparoscopic seromuscular dissection technique. Dig Surg. 2010;27:461–465. - PubMed
-
- Meza JM, Wong SL. Surgical options for advanced/metastatic gastrointestinal stromal tumors. Curr Probl Cancer. 2011;35:283–293. - PubMed
-
- Grover S, Ashley SW, Raut CP. Small intestine gastrointestinal stromal tumors. Curr Opin Gastroenterol. 2012;28:113–123. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
