

QuantiFERON®-TB gold in-tube performance for diagnosing active tuberculosis in children and adults in a high burden setting
- PMID: 22808002
- PMCID: PMC3395691
- DOI: 10.1371/journal.pone.0037851
QuantiFERON®-TB gold in-tube performance for diagnosing active tuberculosis in children and adults in a high burden setting
Abstract
Aim: To determine whether QuantiFERON®-TB Gold In-Tube (QFT) can contribute to the diagnosis of active tuberculosis (TB) in children in a high-burden setting and to assess the performance of QFT and tuberculin skin test (TST) in a prospective cohort of TB suspect children compared to adults with confirmed TB in Tanzania.
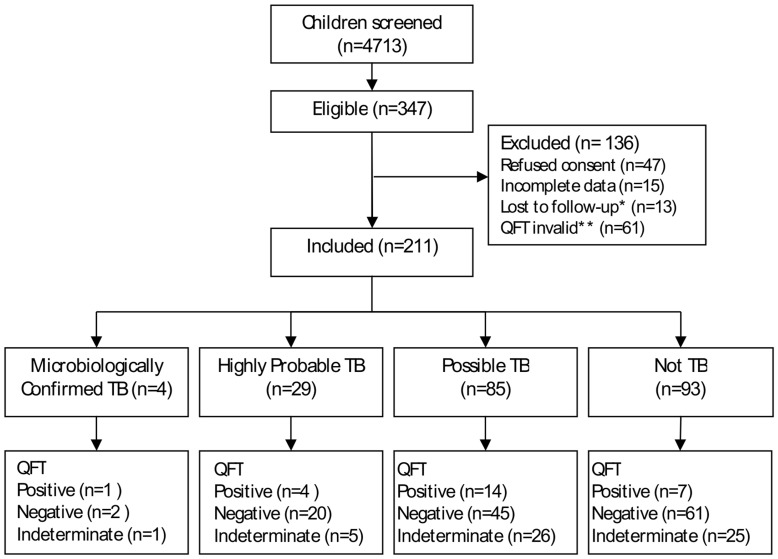
Methods: Sensitivity and specificity of QFT and TST for diagnosing active TB as well as indeterminate QFT rates and IFN-γ levels were assessed in 211 TB suspect children in a Tanzanian district hospital and contrasted in 90 adults with confirmed pulmonary TB.
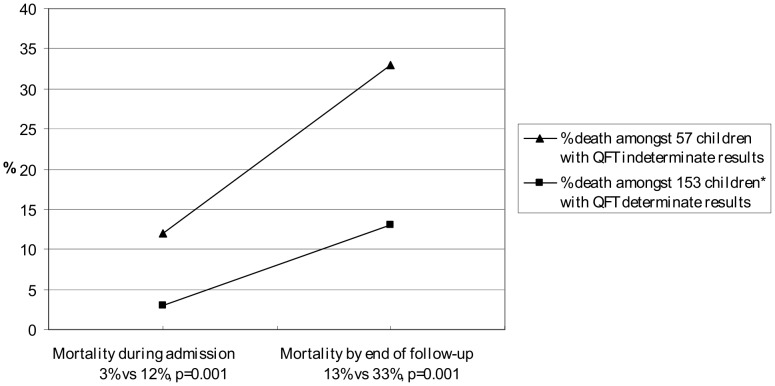
Results: Sensitivity of QFT and TST in children with confirmed TB was 19% (5/27) and 6% (2/31) respectively. In adults sensitivity of QFT and TST was 84% (73/87) and 85% (63/74). The QFT indeterminate rate in children and adults was 27% and 3%. Median levels of IFN-γ were lower in children than adults, particularly children <2 years and HIV infected. An indeterminate result was associated with age <2 years but not malnutrition or HIV status. Overall childhood mortality was 19% and associated with an indeterminate QFT result at baseline.
Conclusion: QFT and TST showed poor performance and a surprisingly low sensitivity in children. In contrast the performance in Tanzanian adults was good and comparable to performance in high-income countries. Indeterminate results in children were associated with young age and increased mortality. Neither test can be recommended for diagnosing active TB in children with immature or impaired immunity in a high-burden setting.
Conflict of interest statement
Figures
References
-
- Chintu C, Mudenda V, Lucas S, Nunn A, Lishimpi K, et al. Lung diseases at necropsy in African children dying from respiratory illnesses: a descriptive necropsy study. Lancet 360: 985–990. S0140–6736(02)11082–8 [pii];10.1016/S0140–6736(02)11082–8 [doi] 2002. - PubMed
-
- McNally LM, Jeena PM, Gajee K, Thula SA, Sturm AW, et al. Effect of age, polymicrobial disease, and maternal HIV status on treatment response and cause of severe pneumonia in South African children: a prospective descriptive study. Lancet 369: 1440–1451. S0140–6736(07)60670–9 [pii];10.1016/S0140–6736(07)60670–9 [doi] 2007. - PubMed
-
- Marais BJ, Gie RP, Schaaf HS, Beyers N, Donald PR, et al. Childhood pulmonary tuberculosis: old wisdom and new challenges. Am J Respir Crit Care Med 173: 1078–1090. 200511–1809SO [pii];10.1164/rccm.200511–1809SO [doi] 2006. - PubMed
-
- WHO/HTM/TB/2006/371. Guidance for national tubeculosis programmes on the management of tuberculosis in children. 2006. - PubMed
-
- Van RP. The use of the paediatric tuberculosis score chart in an HIV-endemic area. Trop Med Int Health 7: 435–441. 882 [pii] 2002. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
