

Radical prostatectomy versus observation for localized prostate cancer
- PMID: 22808955
- PMCID: PMC3429335
- DOI: 10.1056/NEJMoa1113162
Radical prostatectomy versus observation for localized prostate cancer
Erratum in
- N Engl J Med. 2012 Aug 9;367(6):582
Abstract
Background: The effectiveness of surgery versus observation for men with localized prostate cancer detected by means of prostate-specific antigen (PSA) testing is not known.
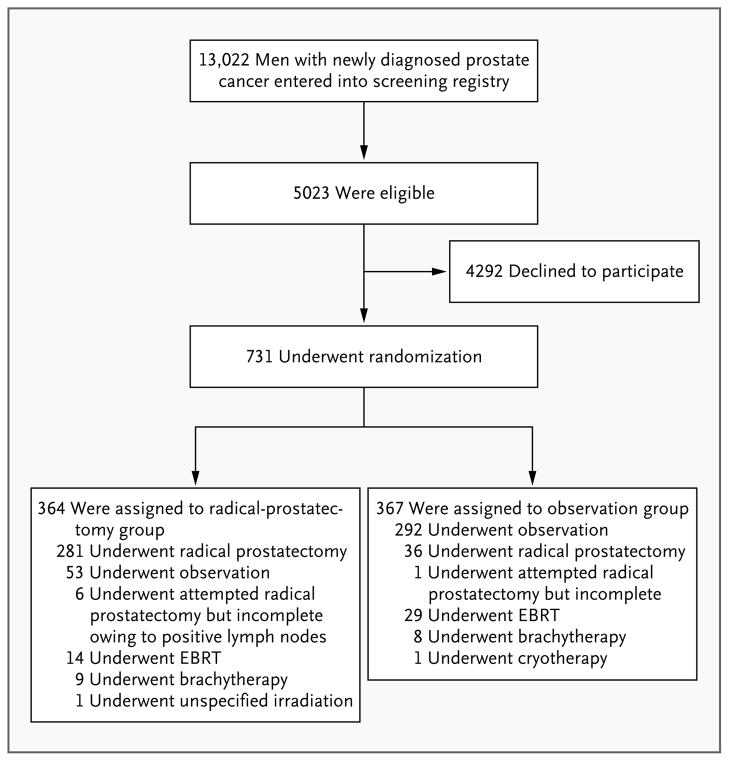
Methods: From November 1994 through January 2002, we randomly assigned 731 men with localized prostate cancer (mean age, 67 years; median PSA value, 7.8 ng per milliliter) to radical prostatectomy or observation and followed them through January 2010. The primary outcome was all-cause mortality; the secondary outcome was prostate-cancer mortality.
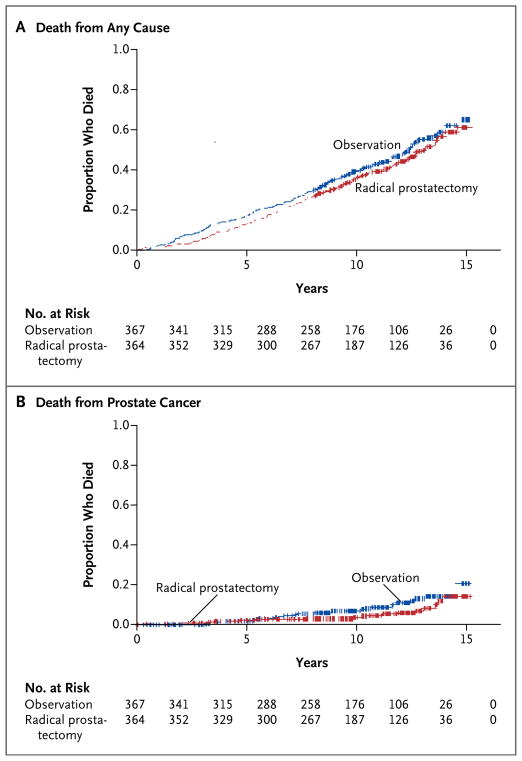
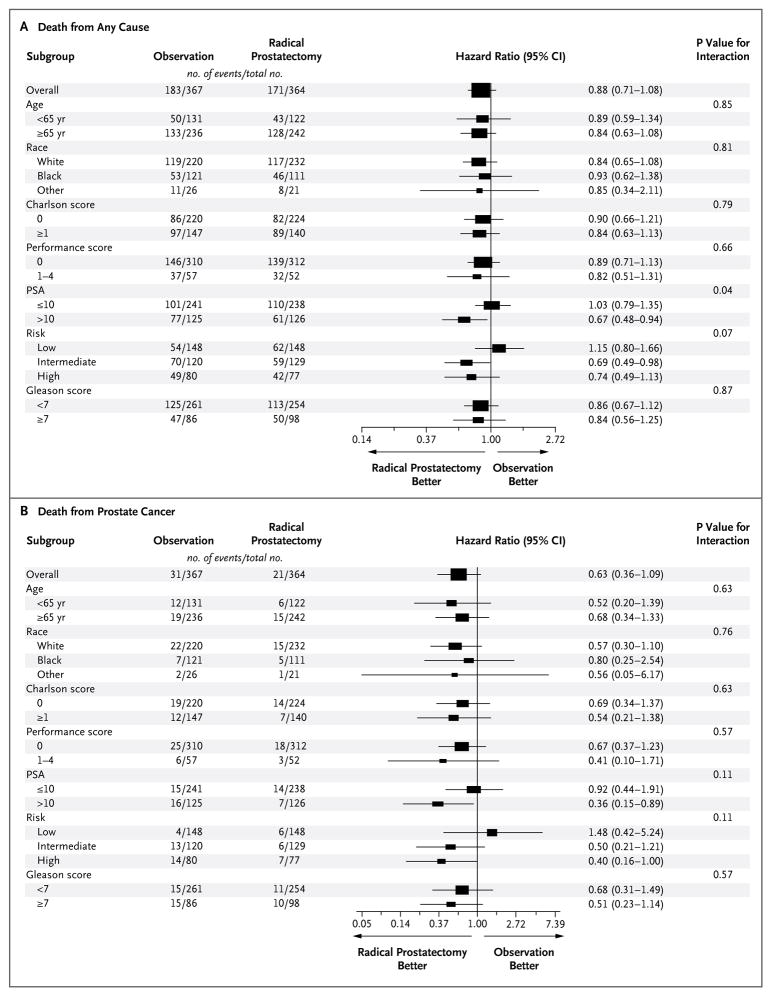
Results: During the median follow-up of 10.0 years, 171 of 364 men (47.0%) assigned to radical prostatectomy died, as compared with 183 of 367 (49.9%) assigned to observation (hazard ratio, 0.88; 95% confidence interval [CI], 0.71 to 1.08; P=0.22; absolute risk reduction, 2.9 percentage points). Among men assigned to radical prostatectomy, 21 (5.8%) died from prostate cancer or treatment, as compared with 31 men (8.4%) assigned to observation (hazard ratio, 0.63; 95% CI, 0.36 to 1.09; P=0.09; absolute risk reduction, 2.6 percentage points). The effect of treatment on all-cause and prostate-cancer mortality did not differ according to age, race, coexisting conditions, self-reported performance status, or histologic features of the tumor. Radical prostatectomy was associated with reduced all-cause mortality among men with a PSA value greater than 10 ng per milliliter (P=0.04 for interaction) and possibly among those with intermediate-risk or high-risk tumors (P=0.07 for interaction). Adverse events within 30 days after surgery occurred in 21.4% of men, including one death.
Conclusions: Among men with localized prostate cancer detected during the early era of PSA testing, radical prostatectomy did not significantly reduce all-cause or prostate-cancer mortality, as compared with observation, through at least 12 years of follow-up. Absolute differences were less than 3 percentage points. (Funded by the Department of Veterans Affairs Cooperative Studies Program and others; PIVOT ClinicalTrials.gov number, NCT00007644.).
Conflict of interest statement
No other potential conflict of interest relevant to this article was reported.
Figures
Comment in
-
Prostate cancer--uncertainty and a way forward.N Engl J Med. 2012 Jul 19;367(3):270-1. doi: 10.1056/NEJMe1205012. N Engl J Med. 2012. PMID: 22808963 No abstract available.
-
Urological cancer: Radical lessons learnt from the prostate cancer PIVOT trial.Nat Rev Clin Oncol. 2012 Sep;9(9):489. doi: 10.1038/nrclinonc.2012.133. Epub 2012 Jul 31. Nat Rev Clin Oncol. 2012. PMID: 22850754 No abstract available.
-
Implications of the prostate intervention versus observation trial (PIVOT).Asian J Androl. 2012 Nov;14(6):803-4. doi: 10.1038/aja.2012.93. Epub 2012 Sep 10. Asian J Androl. 2012. PMID: 22960947 Free PMC article.
-
Commentary on: Radical prostatectomy versus observation for localized prostate cancer.Urology. 2012 Dec;80(6):1181-2. doi: 10.1016/j.urology.2012.07.055. Epub 2012 Oct 4. Urology. 2012. PMID: 23040196 No abstract available.
-
Radical prostatectomy versus observation for prostate cancer.N Engl J Med. 2012 Oct 11;367(15):1467; author reply 1468-9. doi: 10.1056/NEJMc1209800. N Engl J Med. 2012. PMID: 23050531 No abstract available.
-
Radical prostatectomy versus observation for prostate cancer.N Engl J Med. 2012 Oct 11;367(15):1467-8; author reply 1468-9. doi: 10.1056/NEJMc1209800. N Engl J Med. 2012. PMID: 23050532 No abstract available.
-
Radical prostatectomy versus observation for prostate cancer.N Engl J Med. 2012 Oct 11;367(15):1468; author reply 1468-9. doi: 10.1056/NEJMc1209800. N Engl J Med. 2012. PMID: 23050533 No abstract available.
-
Radical prostatectomy versus observation for prostate cancer.N Engl J Med. 2012 Oct 11;367(15):1468; author reply 1468-9. doi: 10.1056/NEJMc1209800. N Engl J Med. 2012. PMID: 23050534 No abstract available.
-
ACP Journal Club. Radical prostatectomy and observation did not differ for mortality in localized prostate cancer.Ann Intern Med. 2012 Oct 16;157(8):JC4-5. doi: 10.7326/0003-4819-157-8-201210160-02005. Ann Intern Med. 2012. PMID: 23070507 No abstract available.
-
Radical prostatectomy does not improve survival compared to observation for localised prostate cancer in a prospective randomised trial.Evid Based Med. 2013 Aug;18(4):139-40. doi: 10.1136/eb-2012-100994. Epub 2012 Oct 20. Evid Based Med. 2013. PMID: 23086567 No abstract available.
-
[Radical prostatectomy versus observation for localized prostate cancer].Strahlenther Onkol. 2012 Dec;188(12):1159-60. doi: 10.1007/s00066-012-0246-5. Strahlenther Onkol. 2012. PMID: 23108386 German. No abstract available.
-
Words of wisdom. Re: Radical prostatectomy versus observation for localized prostate cancer.Eur Urol. 2012 Dec;62(6):1195. doi: 10.1016/j.eururo.2012.09.015. Eur Urol. 2012. PMID: 23141124 No abstract available.
-
Words of wisdom. Re: Radical prostatectomy versus observation for localized prostate cancer.Eur Urol. 2012 Dec;62(6):1196. doi: 10.1016/j.eururo.2012.09.016. Eur Urol. 2012. PMID: 23141125 No abstract available.
-
Re: Radical prostatectomy versus observation for localized prostate cancer.J Urol. 2012 Dec;188(6):2225-6. doi: 10.1016/j.juro.2012.09.067. Epub 2012 Oct 22. J Urol. 2012. PMID: 23141224 No abstract available.
-
Words of wisdom: re: radical prostatectomy versus observation for localized prostate cancer.Eur Urol. 2013 Apr;63(4):767-8. doi: 10.1016/j.eururo.2012.12.053. Eur Urol. 2013. PMID: 23438391 No abstract available.
-
Words of wisdom: re: radical prostatectomy versus observation for localized prostate cancer.Eur Urol. 2013 Apr;63(4):767. doi: 10.1016/j.eururo.2012.12.052. Eur Urol. 2013. PMID: 23438392 No abstract available.
-
Update in general internal medicine: evidence published in 2012.Ann Intern Med. 2013 Apr 16;158(8):615-9. doi: 10.7326/0003-4819-158-8-201304160-00101. Ann Intern Med. 2013. PMID: 23579948 No abstract available.
-
Words of wisdom. Re: Radical prostatectomy versus observation for localized prostate cancer.Eur Urol. 2013 Jun;63(6):1130-1. doi: 10.1016/j.eururo.2013.03.020. Eur Urol. 2013. PMID: 23608081 No abstract available.
-
Prostate cancer: treat or not treat?Actas Urol Esp. 2013 Jul-Aug;37(7):451-2. doi: 10.1016/j.acuro.2013.02.001. Epub 2013 Apr 25. Actas Urol Esp. 2013. PMID: 23623362 English, Spanish. No abstract available.
-
[Radical prostatectomy versus observation for localized prostate cancer].Rev Clin Esp (Barc). 2013 Apr;213(3):164. doi: 10.1016/j.rce.2012.12.012. Rev Clin Esp (Barc). 2013. PMID: 23700595 Spanish. No abstract available.
References
-
- Wilt TJ, MacDonald R, Rutks I, Shamliyan TA, Taylor BC, Kane RL. Systematic review: comparative effectiveness and harms of treatments for clinically localized prostate cancer. Ann Intern Med. 2008;148:435–48. [Erratum, Ann Intern Med 2008;148:888.] - PubMed
-
- Thompson I, Thrasher JB, Aus G, et al. Guideline for the management of clinically localized prostate cancer: 2007 update. Linthicum, MD: American Urological Association Education and Research; 2007. ( http://www.auanet.org/content/clinical-practice-guidelines/clinical-guid...)
-
- SEER cancer statistics review 1975–2004. Bethesda, MD: National Cancer Institute; 2007. ( http://seer.cancer.gov/csr/1975_2004)
-
- Iversen P, Madsen PO, Corle DK. Radical prostatectomy versus expectant treatment for early carcinoma of the prostate: twenty-three year follow-up of a prospective randomized study. Scand J Urol Nephrol Suppl. 1995;172:65–72. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous