

Value of soluble TREM-1, procalcitonin, and C-reactive protein serum levels as biomarkers for detecting bacteremia among sepsis patients with new fever in intensive care units: a prospective cohort study
- PMID: 22809118
- PMCID: PMC3426475
- DOI: 10.1186/1471-2334-12-157
Value of soluble TREM-1, procalcitonin, and C-reactive protein serum levels as biomarkers for detecting bacteremia among sepsis patients with new fever in intensive care units: a prospective cohort study
Abstract
Background: The purpose of this study was to explore the diagnostic value of soluble triggering receptor expressed on myeloid cells 1 (sTREM-1), procalcitonin (PCT), and C-reactive protein (CRP) serum levels for differentiating sepsis from SIRS, identifying new fever caused by bacteremia, and assessing prognosis when new fever occurred.
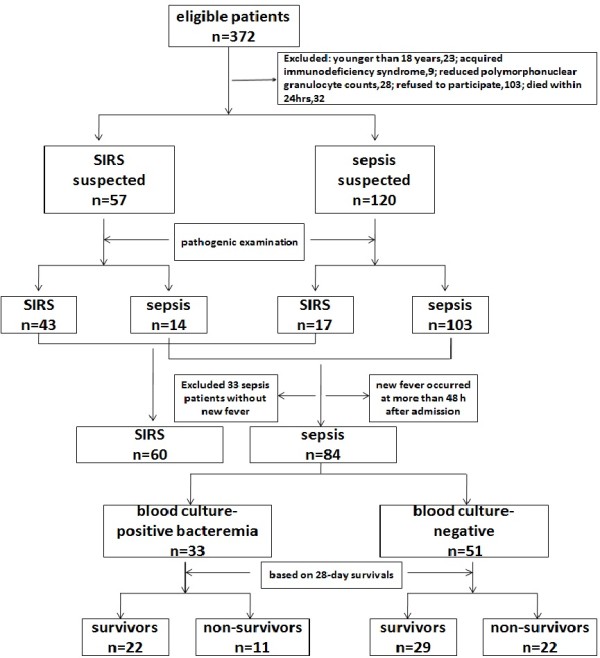
Methods: We enrolled 144 intensive care unit (ICU) patients: 60 with systemic inflammatory response syndrome (SIRS) and 84 with sepsis complicated by new fever at more than 48 h after ICU admission. Serum sTREM-1, PCT, and CRP levels were measured on the day of admission and at the occurrence of new fever (>38.3°C) during hospitalization. Based on the blood culture results, the patients were divided into a blood culture-positive bacteremia group (33 patients) and blood culture-negative group (51 patients). Based on 28-day survival, all patients, both blood culture-positive and -negative, were further divided into survivor and nonsurvivor groups.
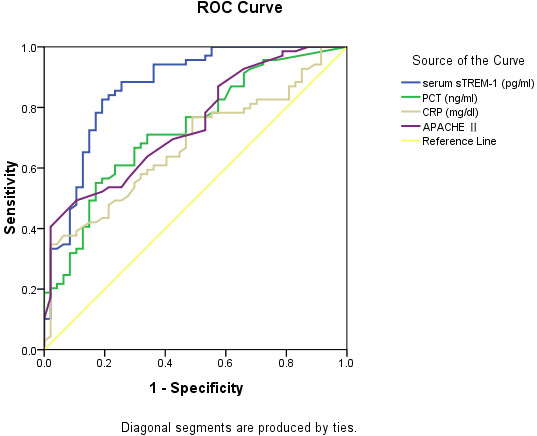
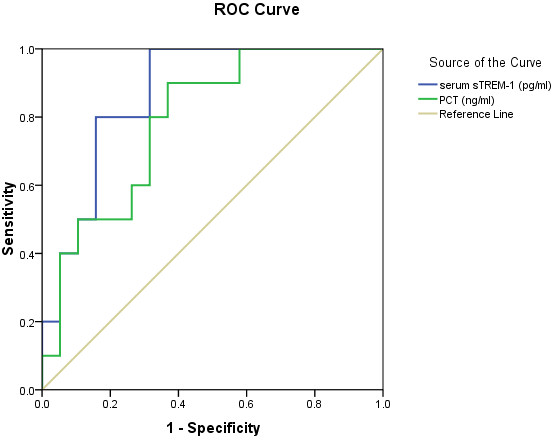
Results: On ICU day 1, the sepsis group had higher serum sTREM-1, PCT, and CRP levels compared with the SIRS group (P <0.05). The areas under the curve (AUC) for these indicators were 0.868 (95% CI, 0.798-0.938), 0.729 (95% CI, 0.637-0.821), and 0.679 (95% CI, 0.578-0.771), respectively. With 108.9 pg/ml as the cut-off point for serum sTREM-1, sensitivity was 0.83 and specificity was 0.81. There was no statistically significant difference in serum sTREM-1 or PCT levels between the blood culture-positive and -negative bacteremia groups with ICU-acquired new fever. However, the nonsurvivors in the blood culture-positive bacteremia group had higher levels of serum sTREM-1 and PCT (P <0.05), with a prognostic AUC for serum sTREM-1 of 0.868 (95% CI, 0.740-0.997).
Conclusions: Serum sTREM-1, PCT, and CRP levels each have a role in the early diagnosis of sepsis. Serum sTREM-1, with the highest sensitivity and specificity of all indicators studied, is especially notable. sTREM-1, PCT, and CRP levels are of no use in determining new fever caused by bacteremia in ICU patients, but sTREM-1 levels reflect the prognosis of bacteremia.
Trial registration: ClinicalTrial.gov identifier NCT01410578.
Figures


Similar articles
-
Dynamic changes of serum soluble triggering receptor expressed on myeloid cells-1 (sTREM-1) reflect sepsis severity and can predict prognosis: a prospective study.BMC Infect Dis. 2011 Mar 1;11:53. doi: 10.1186/1471-2334-11-53. BMC Infect Dis. 2011. PMID: 21356122 Free PMC article.
-
Serum soluble triggering receptor expressed on myeloid cells-1 and procalcitonin can reflect sepsis severity and predict prognosis: a prospective cohort study.Mediators Inflamm. 2014;2014:641039. doi: 10.1155/2014/641039. Epub 2014 Feb 4. Mediators Inflamm. 2014. PMID: 24672147 Free PMC article.
-
Diagnostic value of dynamics serum sCD163, sTREM-1, PCT, and CRP in differentiating sepsis, severity assessment, and prognostic prediction.Mediators Inflamm. 2013;2013:969875. doi: 10.1155/2013/969875. Epub 2013 Jul 1. Mediators Inflamm. 2013. PMID: 23935252 Free PMC article.
-
PCT and sTREM-1: the markers of infection in critically ill patients?Med Sci Monit. 2008 Dec;14(12):RA241-7. Med Sci Monit. 2008. PMID: 19043381 Review.
-
Rapid diagnosis of sepsis.Virulence. 2014 Jan 1;5(1):154-60. doi: 10.4161/viru.27393. Epub 2013 Dec 11. Virulence. 2014. PMID: 24335467 Free PMC article. Review.
Cited by
-
TREM-1 as a potential therapeutic target in neonatal sepsis.Int J Clin Exp Med. 2014 Jul 15;7(7):1650-8. eCollection 2014. Int J Clin Exp Med. 2014. PMID: 25126161 Free PMC article.
-
Comparative Study of Plasma Endotoxin with Procalcitonin Levels in Diagnosis of Bacteremia in Intensive Care Unit Patients.Chin Med J (Engl). 2016 Feb 20;129(4):417-23. doi: 10.4103/0366-6999.176064. Chin Med J (Engl). 2016. PMID: 26879015 Free PMC article.
-
Biomarkers for Sepsis: What Is and What Might Be?Biomark Insights. 2015 Sep 15;10(Suppl 4):7-17. doi: 10.4137/BMI.S29519. eCollection 2015. Biomark Insights. 2015. PMID: 26417200 Free PMC article. Review.
-
Soluble TREM-1 Serum Level can Early Predict Mortality of Patients with Sepsis, Severe Sepsis and Septic Shock.Arch Immunol Ther Exp (Warsz). 2018 Aug;66(4):299-306. doi: 10.1007/s00005-017-0499-x. Epub 2017 Dec 27. Arch Immunol Ther Exp (Warsz). 2018. PMID: 29282483 Free PMC article.
-
Diagnostic Value of Endotracheal Tube-Aspirate Soluble Triggering Receptor Expressed on Myeloid Cells-1 Concentration for Neonatal Ventilator-Associated Pneumonia.Front Pediatr. 2021 Aug 25;9:664801. doi: 10.3389/fped.2021.664801. eCollection 2021. Front Pediatr. 2021. PMID: 34513755 Free PMC article.
References
-
- Bates DW, Sands K, Miller E, Lanken PN, Hibberd PL, Graman PS, Schwartz JS, Kahn K, Snydman DR, Parsonnet J. et al.Predicting bacteremia in patients with sepsis syndrome. Academic Medical Center Consortium Sepsis Project Working Group. J Infect Dis. 1997;176(6):1538–1551. doi: 10.1086/514153. - DOI - PubMed
-
- Weinstein MP, Towns ML, Quartey SM, Mirrett S, Reimer LG, Parmigiani G, Reller LB. The clinical significance of positive blood cultures in the 1990s: a prospective comprehensive evaluation of the microbiology, epidemiology, and outcome of bacteremia and fungemia in adults. Clin Infect Dis. 1997;24(4):584–602. - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
