

The effect of telemedicine in critically ill patients: systematic review and meta-analysis
- PMID: 22809335
- PMCID: PMC3580710
- DOI: 10.1186/cc11429
The effect of telemedicine in critically ill patients: systematic review and meta-analysis
Abstract
Introduction: Telemedicine extends intensivists' reach to critically ill patients cared for by other physicians. Our objective was to evaluate the impact of telemedicine on patients' outcomes.
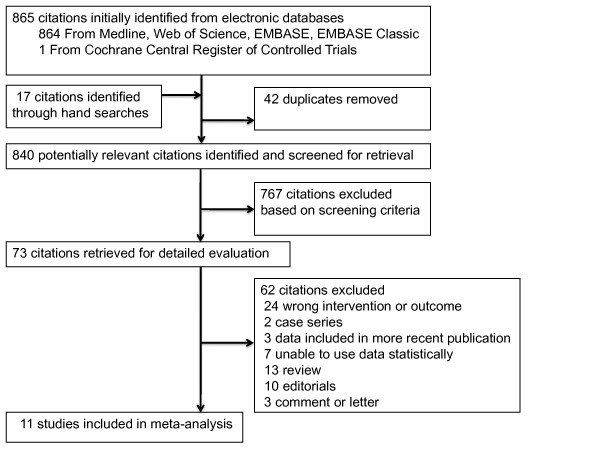
Methods: We searched electronic databases through April 2012, bibliographies of included trials, and indexes and conference proceedings in two journals (2001 to 2012). We selected controlled trials or observational studies of critically ill adults or children, examining the effects of telemedicine on mortality. Two authors independently selected studies and extracted data on outcomes (mortality and length of stay in the intensive care unit (ICU) and hospital) and methodologic quality. We used random-effects meta-analytic models unadjusted for case mix or cluster effects and quantified between-study heterogeneity by using I² (the percentage of total variability across studies attributable to heterogeneity rather than to chance).
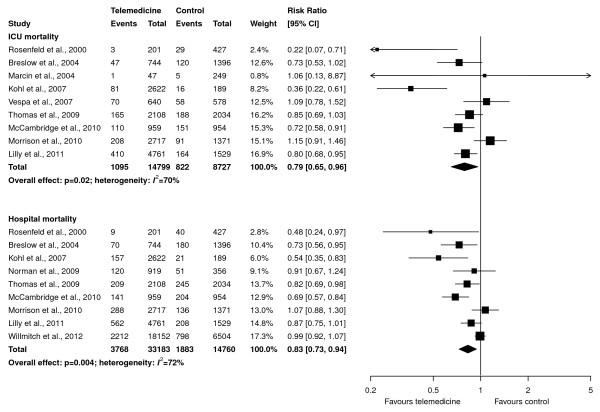
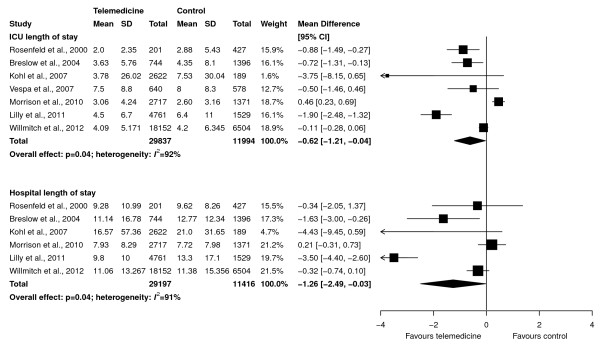
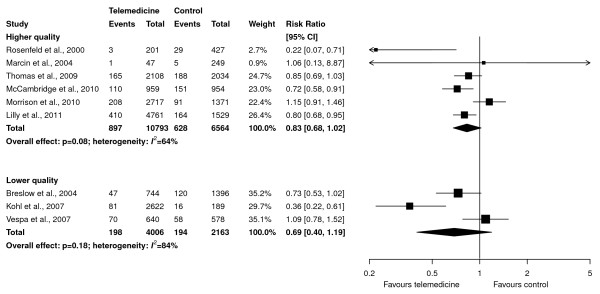
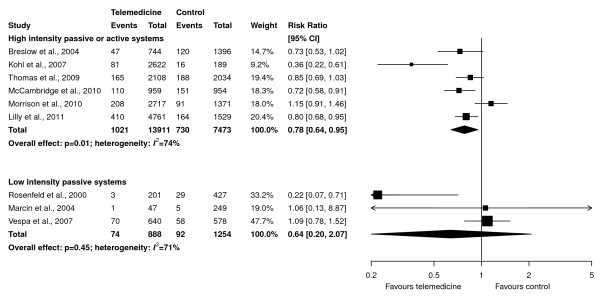
Results: Of 865 citations, 11 observational studies met selection criteria. Overall quality was moderate (mean score on Newcastle-Ottawa scale, 5.1/9; range, 3 to 9). Meta-analyses showed that telemedicine, compared with standard care, is associated with lower ICU mortality (risk ratio (RR) 0.79; 95% confidence interval (CI), 0.65 to 0.96; nine studies, n = 23,526; I2 = 70%) and hospital mortality (RR, 0.83; 95% CI, 0.73 to 0.94; nine studies, n = 47,943; I² = 72%). Interventions with continuous patient-data monitoring, with or without alerts, reduced ICU mortality (RR, 0.78; 95% CI, 0.64 to 0.95; six studies, n = 21,384; I² = 74%) versus those with remote intensivist consultation only (RR, 0.64; 95% CI, 0.20 to 2.07; three studies, n = 2,142; I2 = 71%), but effects were statistically similar (interaction P = 0.74). Effects were also similar in higher (RR, 0.83; 95% CI, 0.68 to 1.02) versus lower (RR, 0.69; 95% CI, 0.40 to 1.19; interaction, P = 0.53) quality studies. Reductions in ICU and hospital length of stay were statistically significant (weighted mean difference (telemedicine-control), -0.62 days; 95% CI, -1.21 to -0.04 days and -1.26 days; 95% CI, -2.49 to -0.03 days, respectively; I2 > 90% for both).
Conclusions: Telemedicine was associated with lower ICU and hospital mortality among critically ill patients, although effects varied among studies and may be overestimated in nonrandomized designs. The optimal telemedicine technology configuration and dose tailored to ICU organization and case mix remain unclear.
Figures
References
-
- Rubenfeld GD, Angus DC. Are intensivists safe? Ann Intern Med. 2008;148:877–879. - PubMed
-
- Angus DC, Kelley MA, Schmitz RJ, White A, Popovich J Jr. (COMPACCS) Caring for the critically ill patient: current and projected workforce requirements for care of the critically ill and patients with pulmonary disease: can we meet the requirements of an aging population? JAMA. 2000;284:2762–2770. doi: 10.1001/jama.284.21.2762. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
