

Serum cystatin C- versus creatinine-based definitions of acute kidney injury following cardiac surgery: a prospective cohort study
- PMID: 22809763
- PMCID: PMC3496012
- DOI: 10.1053/j.ajkd.2012.06.002
Serum cystatin C- versus creatinine-based definitions of acute kidney injury following cardiac surgery: a prospective cohort study
Abstract
Background: The primary aim of this study was to compare the sensitivity and rapidity of acute kidney injury (AKI) detection by cystatin C level relative to creatinine level after cardiac surgery.
Study design: Prospective cohort study.
Settings & participants: 1,150 high-risk adult cardiac surgery patients in the TRIBE-AKI (Translational Research Investigating Biomarker Endpoints for Acute Kidney Injury) Consortium.
Predictor: Changes in serum creatinine and cystatin C levels.
Outcome: Postsurgical incidence of AKI.
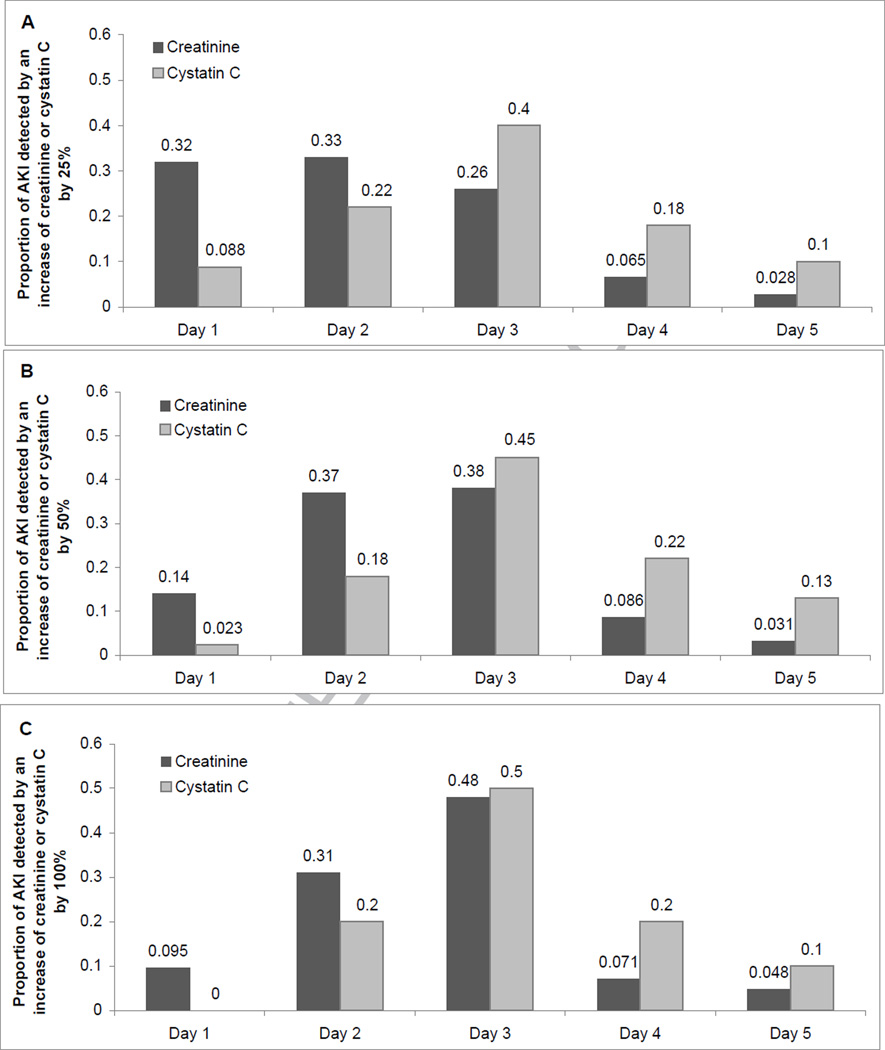
Measurements: Serum creatinine and cystatin C were measured at the preoperative visit and daily on postoperative days 1-5. To allow comparisons between changes in creatinine and cystatin C levels, AKI end points were defined by the relative increases in each marker from baseline (25%, 50%, and 100%) and the incidence of AKI was compared based on each marker. Secondary aims were to compare clinical outcomes among patients defined as having AKI by cystatin C and/or creatinine levels.
Results: Overall, serum creatinine level detected more cases of AKI than cystatin C level: 35% developed a ≥25% increase in serum creatinine level, whereas only 23% had a ≥25% increase in cystatin C level (P < 0.001). Creatinine level also had higher proportions meeting the 50% (14% and 8%; P < 0.001) and 100% (4% and 2%; P = 0.005) thresholds for AKI diagnosis. Clinical outcomes generally were not statistically different for AKI cases detected by creatinine or cystatin C level. However, for each AKI threshold, patients with AKI confirmed by both markers had a significantly higher risk of the combined mortality/dialysis outcome compared with patients with AKI detected by creatinine level alone (P = 0.002).
Limitations: There were few adverse clinical outcomes, limiting our ability to detect differences in outcomes between subgroups of patients based on their definitions of AKI.
Conclusions: In this large multicenter study, we found that cystatin C level was less sensitive for AKI detection than creatinine level. However, confirmation by cystatin C level appeared to identify a subset of patients with AKI with a substantially higher risk of adverse outcomes.
Published by Elsevier Inc.
Figures
References
-
- Chertow GM, Lazarus JM, Christiansen CL, et al. Preoperative renal risk stratification. Circulation. 1997;95:878–884. - PubMed
-
- Thakar CV, Arrigain S, Worley S, Yared JP, Paganini EP. A clinical score to predict acute renal failure after cardiac surgery. J Am Soc Nephrol. 2005;16:162–168. - PubMed
-
- Brown JR, Cochran RP, Dacey LJ, et al. Perioperative increases in serum creatinine are predictive of increased 90-day mortality after coronary artery bypass graft surgery. Circulation. 2006;114:I409–I413. - PubMed
-
- Chertow GM, Levy EM, Hammermeister KE, Grover F, Daley J. Independent association between acute renal failure and mortality following cardiac surgery. Am J Med. 1998;104:343–348. - PubMed
-
- Loef BG, Epema AH, Smilde TD, et al. Immediate postoperative renal function deterioration in cardiac surgical patients predicts in-hospital mortality and long-term survival. J Am Soc Nephrol. 2005;16:195–200. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
