

Two septic transfusion reactions presenting as transfusion-related acute lung injury from a split plateletpheresis unit
- PMID: 22809916
- PMCID: PMC3733455
- DOI: 10.1097/CCM.0b013e3182544f85
Two septic transfusion reactions presenting as transfusion-related acute lung injury from a split plateletpheresis unit
Abstract
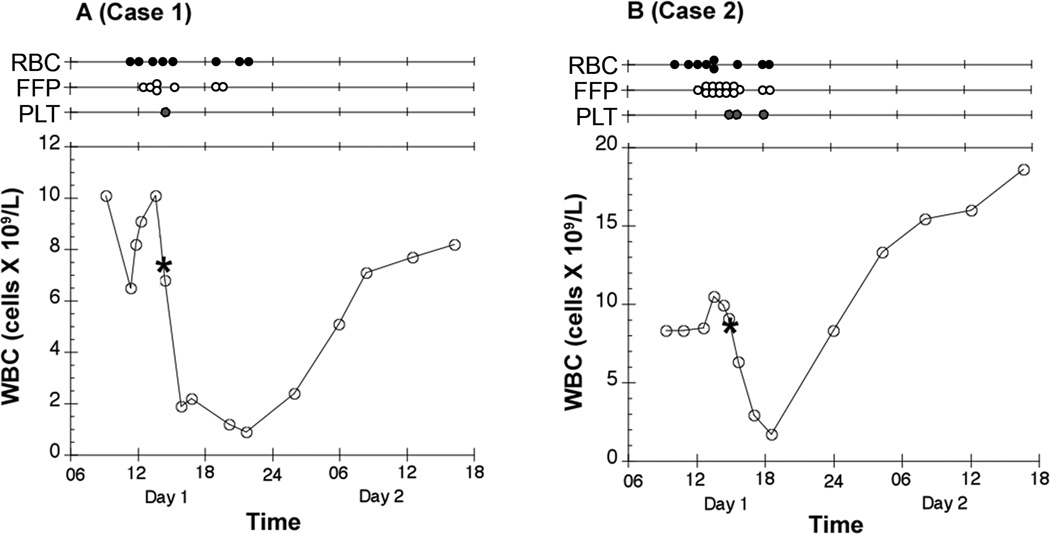
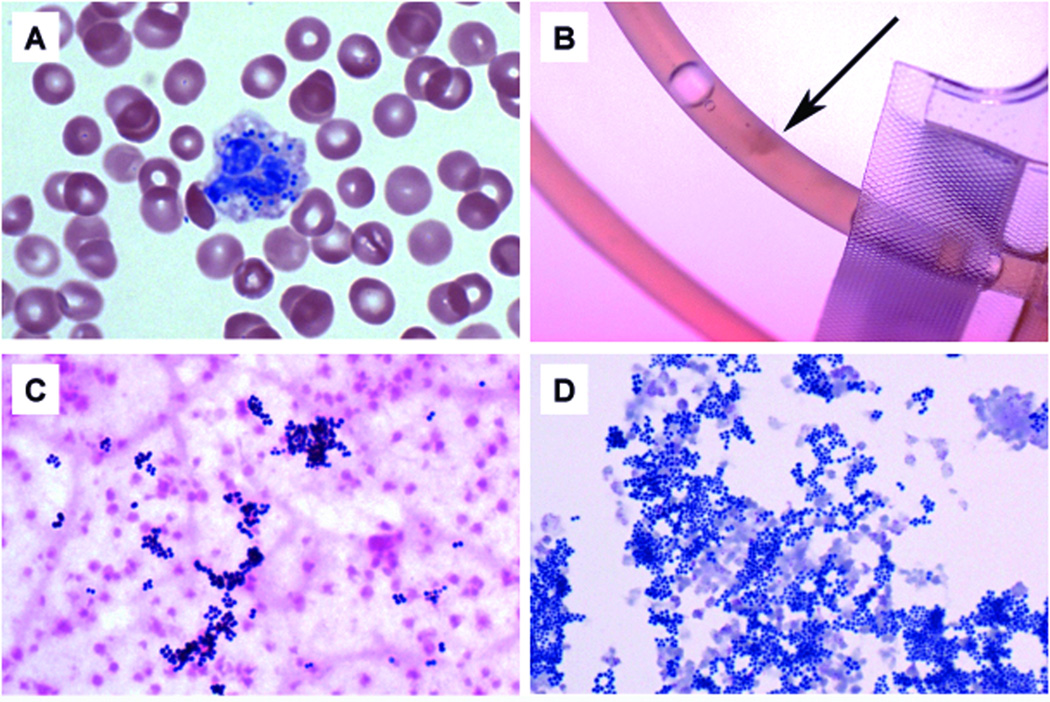
Objectives: We report two simultaneous cases of Staphylococcus aureus sepsis initially consistent with and diagnosed as transfusion-related acute lung injury. The sepsis in both cases resulted from transfusion of two split products from a single contaminated plateletpheresis unit. In each case, the platelets were given along with numerous other blood products during posterior spine surgery. The discussion includes presentation, clinical course, diagnosis, and similarities between sepsis and transfusion-related acute lung injury. The cases and discussion highlight the importance of considering sepsis as part of the differential for any patient believed to have transfusion-related acute lung injury with clinical features of sepsis.
Data sources: Data were collected from the patients' electronic medical records and the hospital laboratory medicine database.
Conclusions: Our cases highlight the importance of vigilant investigation in patients suspected of transfusion-related acute lung injury, as septic transfusions are easily missed and may mimic or coexist with transfusion-related acute lung injury. Sepsis should be strongly considered whenever clinical features such as hypotension, leucopenia, and fever are noted in patients with suspected transfusion-related acute lung injury. In comparison to patients receiving red blood cells or plasma, platelet transfusion recipients are at a greater risk for sepsis from a contaminated unit. Patients developing sepsis from a contaminated blood product may meet the clinical definition of transfusion-related acute lung injury. In such cases, if the clinical syndrome is attributed solely to transfusion-related acute lung injury and bacterial sepsis is not suspected, the correct diagnosis may be missed or delayed. Consequently, appropriate treatment for sepsis would also be delayed or not provided and likely result in increased morbidity and mortality.
Conflict of interest statement
The authors have not disclosed any potential conflicts of interest
Figures
References
-
- Busch MP, Glynn SA, Stramer SL, et al. A new strategy for estimating risks of transfusion-transmitted viral infections based on rates of detection of recently infected donors. Transfusion. 2005;45(2):254–264. - PubMed
-
- Busch MR. Evolving approaches to estimate risks of transfusion-transmitted viral infections: incidence-window period model after ten years. Dev Biol (Basel) 2007;127:87–112. - PubMed
-
- Zou S, Dorsey KA, Notari EP, et al. Prevalence, incidence, and residual risk of human immunodeficiency virus and hepatitis C virus infections among United States blood donors since the introduction of nucleic acid testing. Transfusion. 2010;50(7):1495–1504. - PubMed
-
- Zou S, Stramer SL, Notari EP, et al. Current incidence and residual risk of hepatitis B infection among blood donors in the United States. Transfusion. 2009 - PubMed
-
- Toy P, Popovsky MA, Abraham E, et al. Transfusion-related acute lung injury: definition and review. Crit Care Med. 2005;33(4):721–726. - PubMed
