

Addition of an induction regimen of antiangiogenesis and antitumor immunity to standard chemotherapy improves survival in advanced malignancies
- PMID: 22810591
- PMCID: PMC3505507
- DOI: 10.1007/s12032-012-0301-1
Addition of an induction regimen of antiangiogenesis and antitumor immunity to standard chemotherapy improves survival in advanced malignancies
Abstract
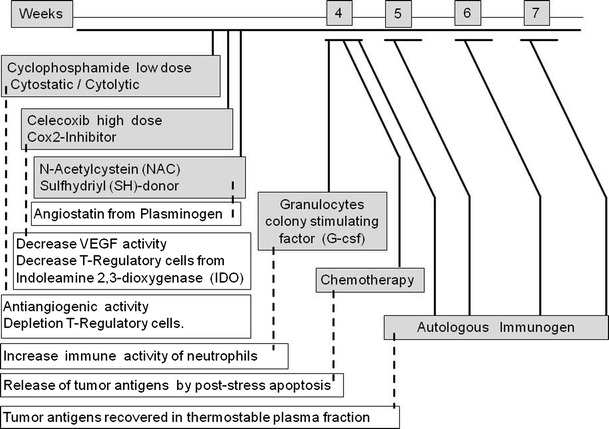
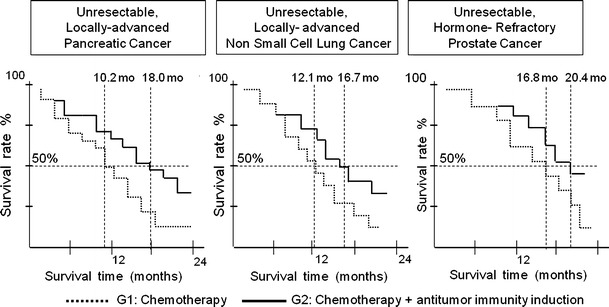
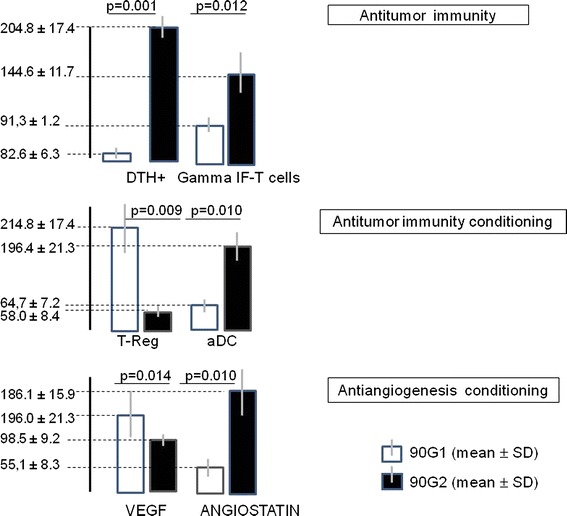
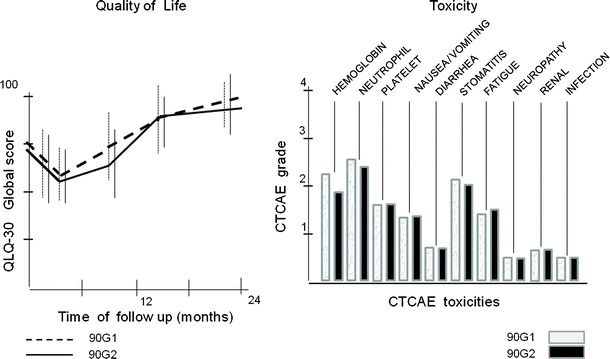
Studies have shown that cancer requires two conditions for tumor progression: cancer cell proliferation and an environment permissive to and conditioned by malignancy. Chemotherapy aims to control the number and proliferation of cancer cells, but it does not effectively control the two best-known conditions of the tumor-permissive environment: neoangiogenesis and tolerogenic immunity. Many malignant diseases exhibit poor outcomes after treatment with chemotherapy. Therefore, we investigated the potential benefits of adding an induction regimen of antiangiogenesis and antitumor immunity to chemotherapy in poor outcome disease. In a prospective, randomized trial, we included patients with advanced, unresectable pancreatic adenocarcinomas, non-small cell lung cancer, or prostate cancer. Two groups of each primary condition were compared: group 1 (G1), n = 30, was treated with the standard chemotherapy and used as a control, and group 2 (G2), n = 30, was treated with chemotherapy plus an induction regimen of antiangiogenesis and antitumor immunity. This induction regimen included a low dose of metronomic cyclophosphamide, a high dose of Cox-2 inhibitor, granulocyte colony-stimulating factor, a sulfhydryl (SH) donor, and a hemoderivative that contained autologous tumor antigens released from patient tumors into the blood. After treatment, the G2 group demonstrated significantly longer survival, lower blood level of neoangiogenesis and immune-tolerance mediators, and higher blood levels of antiangiogenesis and antitumor immunity mediators compared with the G1 group. Toxicity and quality of life were not significantly different between the groups. In conclusion, in several advanced malignancies of different primary localizations, an increase in survival was observed by adding an induction regimen of antiangiogenesis and antitumor immunity to standard chemotherapy.
Figures
References
-
- Lasalvia-Prisco E, Goldschmidt P, Galmarini F, et al. Switch of biological response (angiogenesis and immunity) as target of complementary treatments in malignancy. In: 37th ESMO congress, Vienna 2012, 28 Sept–02 Oct 2012. Accepted.
-
- Miller K, Sweeney CJ, Sledge GW., Jr Redefining the target: chemotherapeutics as antiangiogenics. J Clin Oncol. 2001;19:1195–1206. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Research Materials
