

Techniques of hepatic resection
- PMID: 22811867
- PMCID: PMC3397635
- DOI: 10.3978/j.issn.2078-6891.2012.006
Techniques of hepatic resection
Abstract
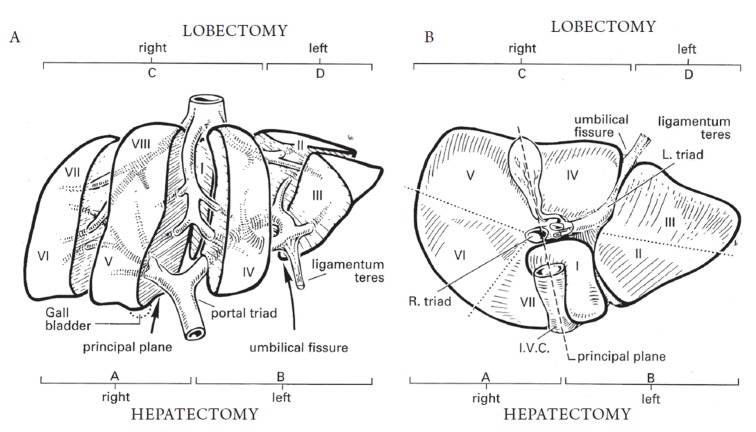
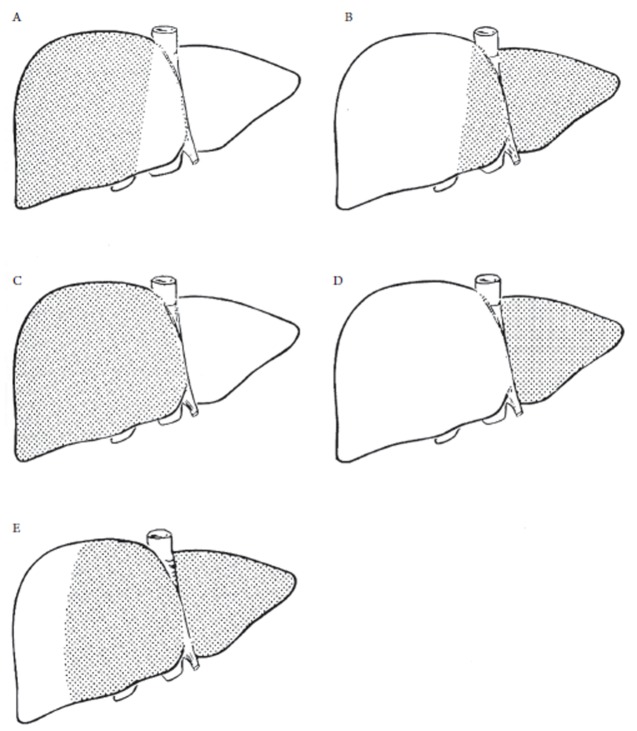
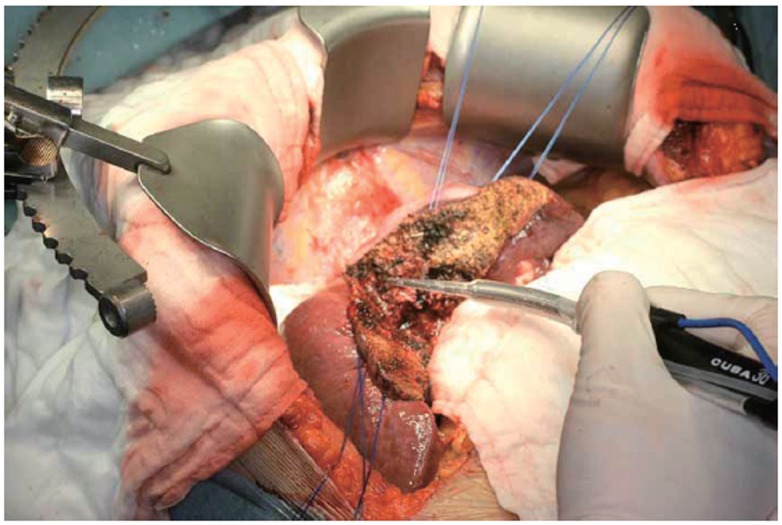
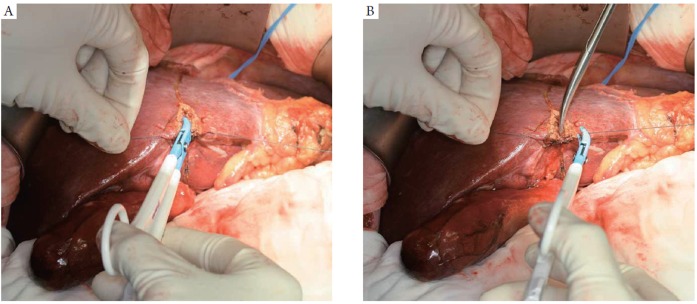
Liver resections are high risk procedures performed by experienced surgeons. The role of liver resection in malignant disease has changed over the last 100 years with great improvement in morbidity, mortality and long term survival. New understanding in liver anatomy, improved perioperative care, anesthesia techniques, and technological advances has improved this aspect of patient care. With improved techniques, patients previously considered unresectable have an opportunity to undergo curative surgery. This review article describes the various approaches and techniques for liver resection. The relevant anatomy and terminology of hepatic resections is discussed, as well as the role of anatomic vs. nonanatomic resection. Methods of vascular control are examined and the multiple strategies of parenchymal transection are compared, as well as minimally-invasive techniques. Finally, a brief review of the authors' practice in terms of surgical technique is offered.
Keywords: Colorectal cancer; liver resection; techniques.
Conflict of interest statement
No potential conflict of interest.
Figures

References
-
- Blumgart LH, Belghiti J. Surgery of the liver, biliary tract, and pancreas. 4th ed. Philadelphia, PA: Saunders Elsevier, 2007.
-
- Skandalakis JE, Skandalakis LJ, Skandalakis PN, Mirilas P. Hepatic surgical anatomy. Surg Clin North Am. 2004;84:413-435. viii. - PubMed
-
- Bismuth H. Surgical anatomy and anatomical surgery of the liver. World J Surg. 1982;6:3-9 - PubMed
-
- Couinaud C. Liver anatomy: portal (and suprahepatic) or biliary segmentation. Dig Surg. 1999;16:459-467 - PubMed
-
- Strasberg SM. Nomenclature of hepatic anatomy and resections: a review of the Brisbane 2000 system. J Hepatobiliary Pancreat Surg. 2005;12:351-355 - PubMed
LinkOut - more resources
Full Text Sources
Molecular Biology Databases