

Comparison of current US risk strategy to screen for hepatitis C virus with a hypothetical targeted birth cohort strategy
- PMID: 22813094
- PMCID: PMC3477967
- DOI: 10.2105/AJPH.2011.300488
Comparison of current US risk strategy to screen for hepatitis C virus with a hypothetical targeted birth cohort strategy
Abstract
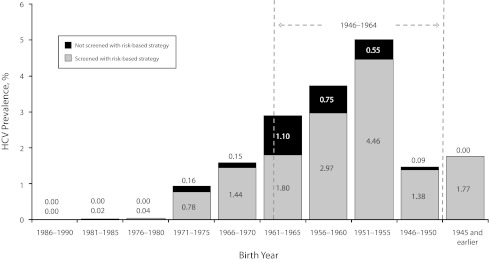
Objectives: We compared the theoretical performance of a 1-time, birth cohort strategy with the currently recommended risk strategy for screening for hepatitis C virus (HCV) infection, which is undetected in an estimated 75% of 4 million affected people in the United States.
Methods: We applied current American Association for the Study of Liver Disease risk screening guidelines and a targeted birth cohort strategy to National Health and Nutrition Examination Survey data from 2003 to 2006 to estimate their performance in identifying HCV cases.
Results: Risk guidelines would recommend testing 25% of the US population aged 20 years or older and, if fully implemented, identify 82% of the projected HCV-exposed population. A targeted birth cohort (1946-1964) strategy would test 45% of the same population and identify 76% of the projected HCV population.
Conclusions: In this ideal-world simulation, birth year and risk screening had similar theoretical performances for predicting HCV infection. However, actual implementation of risk screening has not achieved its theoretical performance, and birth cohort screening might increase HCV testing rates.
Figures
References
-
- Armstrong GL, Wasley A, Simard EP, McQuillan GM, Kuhnert WL, Alter MJ. The prevalence of hepatitis C virus infection in the United States, 1999 through 2002. Ann Intern Med. 2006;144(10):705–714 - PubMed
-
- Davis GL, Alter MJ, El-Serag H, Poynard T, Jennings LW. Aging of hepatitis C virus (HCV)-infected persons in the United States: a multiple cohort model of HCV prevalence and disease progression. Gastroenterology. 2010;138(2):513–521 - PubMed
-
- Alter MJ, Kruszon-Moran D, Nainan OVet al.The prevalence of hepatitis C virus infection in the United States, 1988 through 1994. N Engl J Med. 1999;341(8):556–562 - PubMed
-
- Colvin HM, Mitchell AE. Hepatitis and Liver Cancer: A National Strategy for Prevention and Control of Hepatitis B and C. Washington, DC: National Academies Press; 2010 - PubMed
-
- Pyenson BS, Fitch K, Iwasaki K. Consequences of Hepatitis C Virus (HCV): Costs of a Baby Boomer Epidemic of Liver Disease. New York, NY; 2009
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
