

Reproducibility of histopathological subtypes and invasion in pulmonary adenocarcinoma. An international interobserver study
- PMID: 22814311
- PMCID: PMC5164925
- DOI: 10.1038/modpathol.2012.106
Reproducibility of histopathological subtypes and invasion in pulmonary adenocarcinoma. An international interobserver study
Abstract
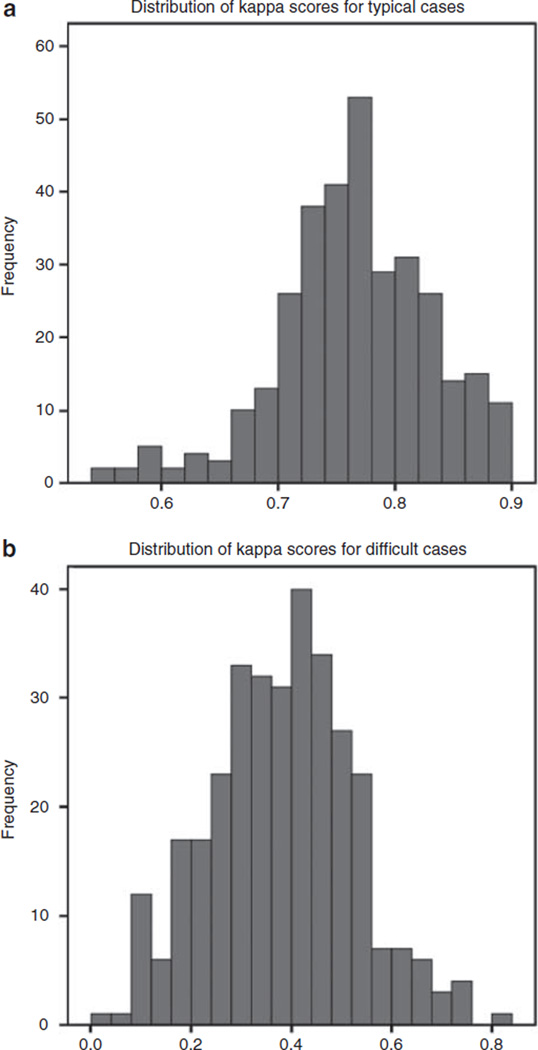
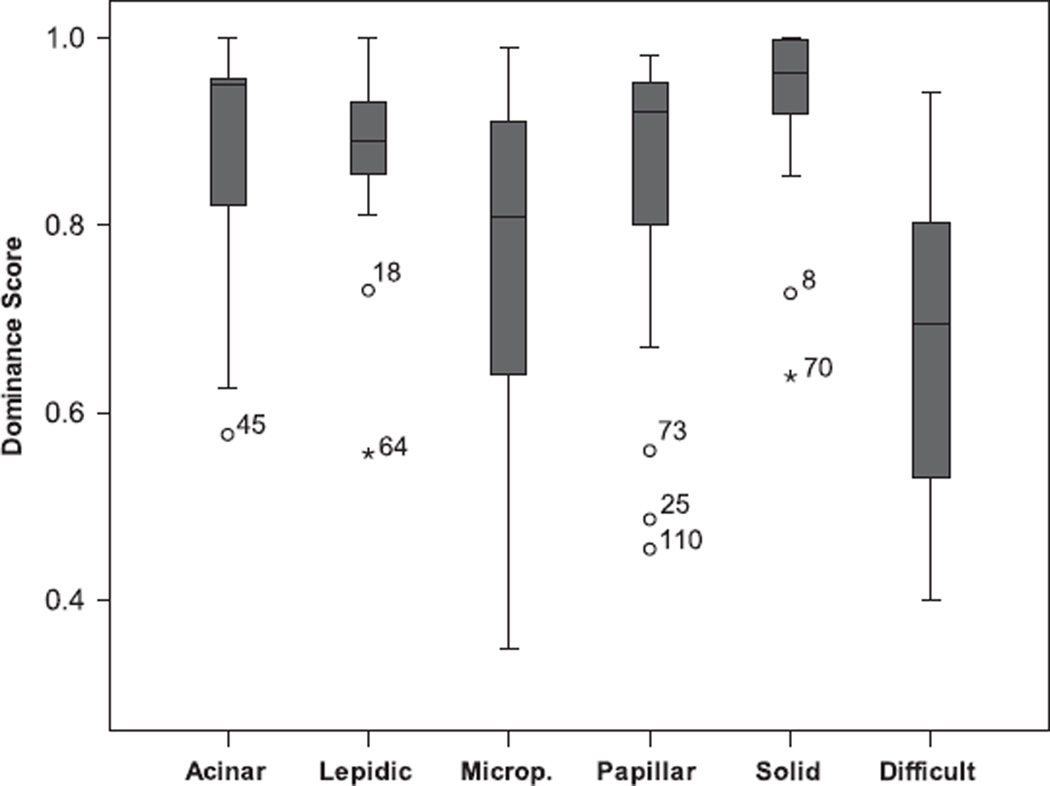
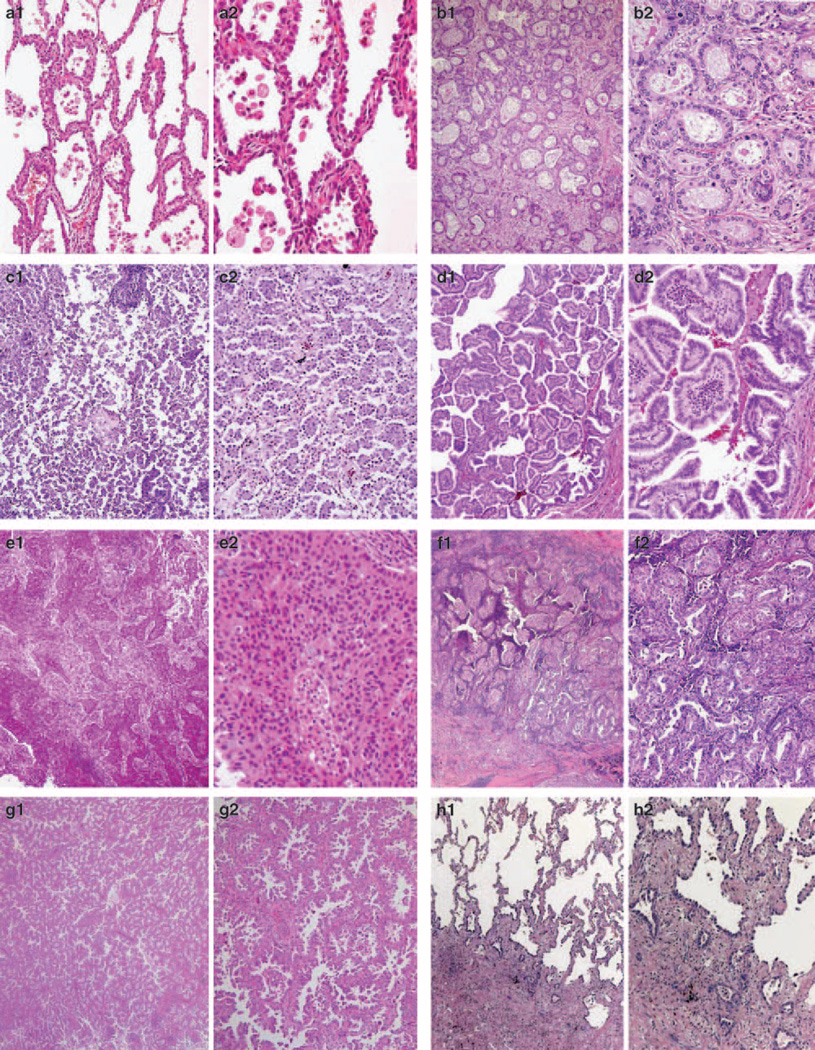
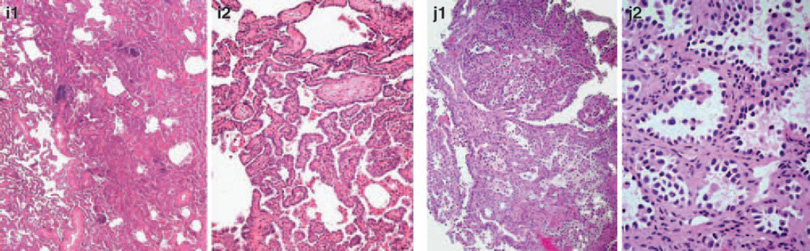
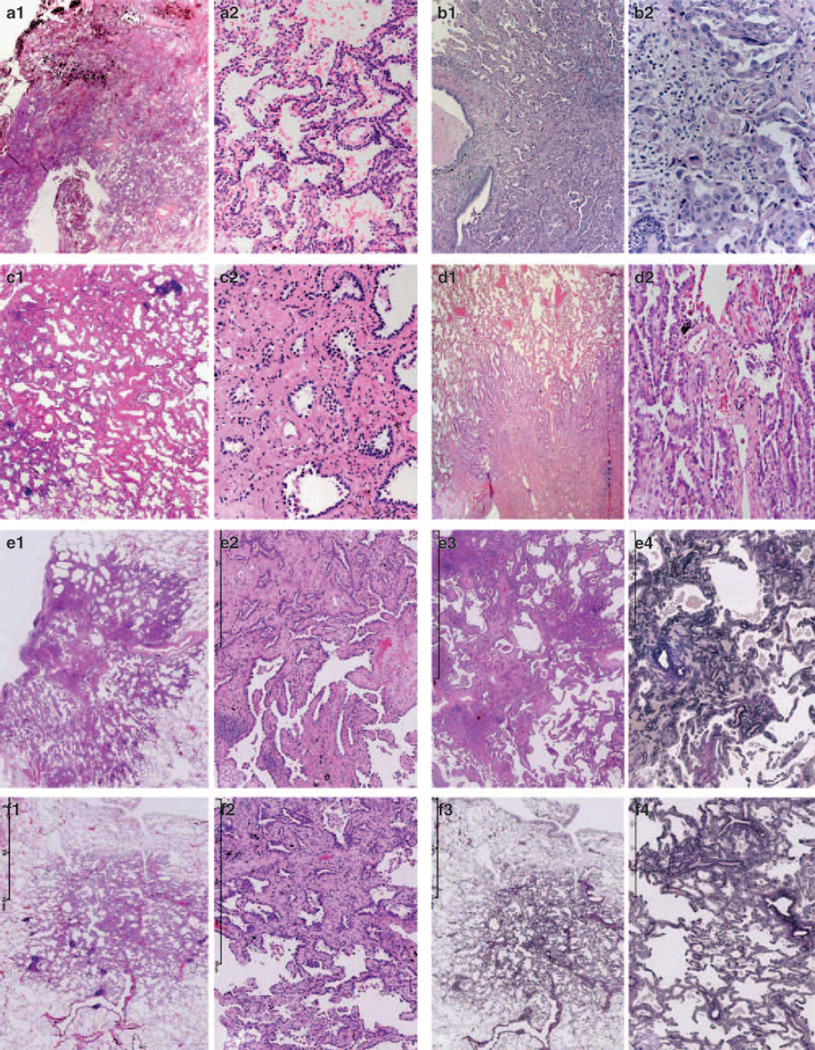
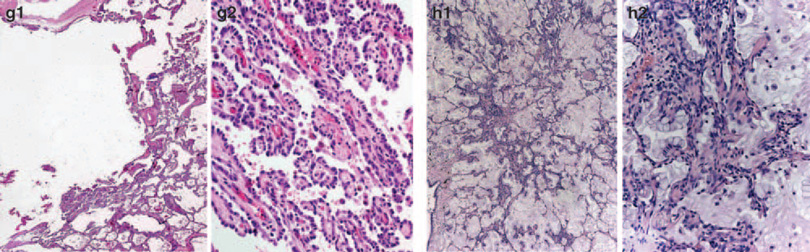
Histological subtyping of pulmonary adenocarcinoma has recently been updated based on predominant pattern, but data on reproducibility are required for validation. This study first assesses reproducibility in subtyping adenocarcinomas and then assesses further the distinction between invasive and non-invasive (wholly lepidic) pattern of adenocarcinoma, among an international group of pulmonary pathologists. Two ring studies were performed using a micro-photographic image-based method, evaluating selected images of lung adenocarcinoma histologic patterns. In the first study, 26 pathologists reviewed representative images of typical and 'difficult' histologic patterns. A total number of scores for the typical patterns combined (n=94) and the difficult cases (n=21) were 2444 and 546, respectively. The mean kappa score (±s.d.) for the five typical patterns combined and for difficult cases were 0.77±0.07 and 0.38±0.14, respectively. Although 70% of the observers identified 12-65% of typical images as single pattern, highest for solid and least for micropapillary, recognizing the predominant pattern was achieved in 92-100%, of the images except for micropapillary pattern (62%). For the second study on invasion, identified as a key problem area from the first study, 28 pathologists submitted and reviewed 64 images representing typical as well as 'difficult' examples. The kappa for typical and difficult cases was 0.55±0.06 and 0.08±0.02, respectively, with consistent subdivision by the same pathologists into invasive and non-invasive categories, due to differing interpretation of terminology defining invasion. In pulmonary adenocarcinomas with classic morphology, which comprise the majority of cases, there is good reproducibility in identifying a predominant pattern and fair reproducibility distinguishing invasive from in-situ (wholly lepidic) patterns. However, more precise definitions and better education on interpretation of existing terminology are required to improve recognition of purely in-situ disease, this being an area of increasing importance.
Conflict of interest statement
Disclosure/conflict of interest The authors declare no conflict of interest.
Figures
References
-
- Travis WD, Brambilla E, Muller-Hermelink KM. Pathology and Genetics: Tumours of the Lung, Pleura, Thymus and Heart. Lyon: IARC; 2004.
-
- Russell PA, Wainer Z, Wright GM, et al. Does lung adenocarcinoma subtype predict patient survival?: A clinicopathologic study based on the new International Association for the Study of Lung Cancer/American Thoracic Society/European Respiratory Society international multidisciplinary lung adenocarcinoma classification. J Thorac Oncol. 2011;6:1496–1504. - PubMed
-
- Yoshizawa A, Motoi N, Riely GJ, et al. Impact of proposed IASLC/ATS/ERS classification of lung adenocarcinoma: prognostic subgroups and implications for further revision of staging based on analysis of 514 stage I cases. Mod Pathol. 2011;24:653–664. - PubMed
-
- Campobasso O, Andrion A, Ribotta M, et al. The value of the 1981 WHO histological classification in interobserver reproducibility and changing pattern of lung cancer. Int J Cancer. 1993;53:205–208. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
