

Effect of a community-based nursing intervention on mortality in chronically ill older adults: a randomized controlled trial
- PMID: 22815653
- PMCID: PMC3398966
- DOI: 10.1371/journal.pmed.1001265
Effect of a community-based nursing intervention on mortality in chronically ill older adults: a randomized controlled trial
Abstract
Background: Improving the health of chronically ill older adults is a major challenge facing modern health care systems. A community-based nursing intervention developed by Health Quality Partners (HQP) was one of 15 different models of care coordination tested in randomized controlled trials within the Medicare Coordinated Care Demonstration (MCCD), a national US study. Evaluation of the HQP program began in 2002. The study reported here was designed to evaluate the survival impact of the HQP program versus usual care up to five years post-enrollment.
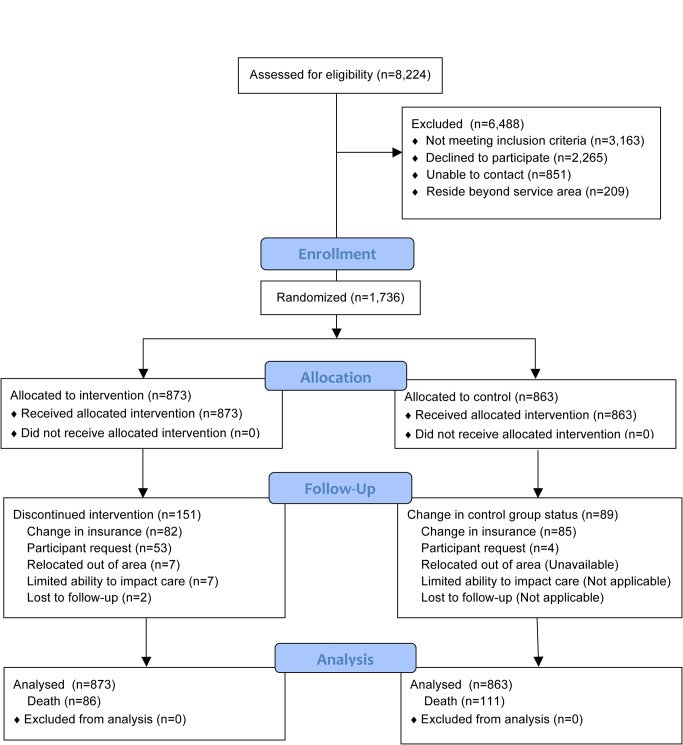
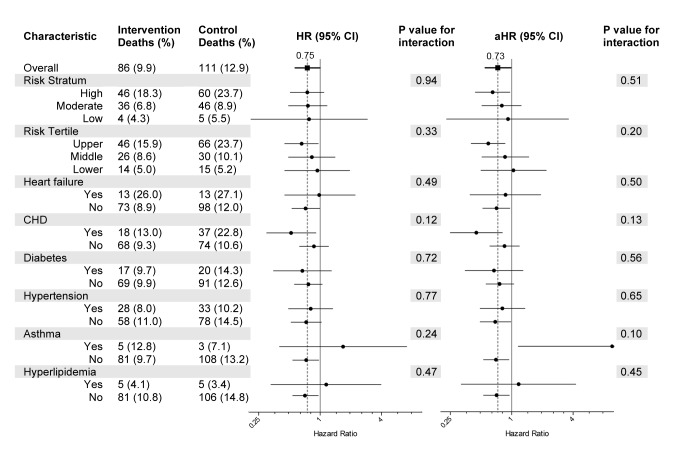
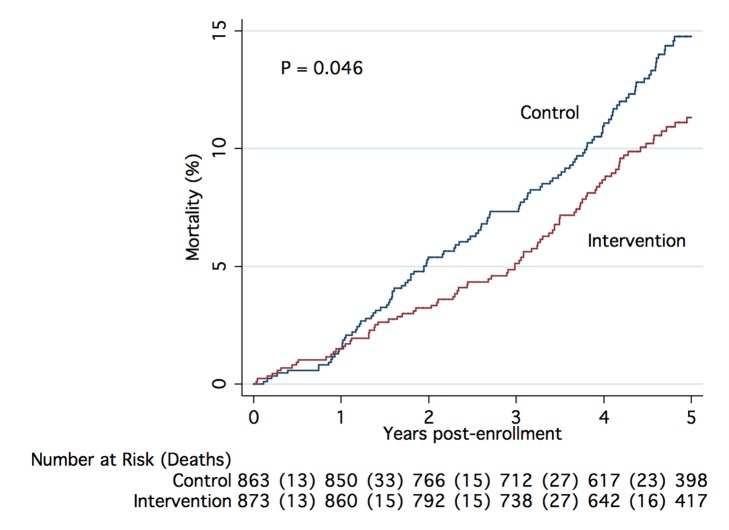
Methods and findings: HQP enrolled 1,736 adults aged 65 and over, with one or more eligible chronic conditions (coronary artery disease, heart failure, diabetes, asthma, hypertension, or hyperlipidemia) during the first six years of the study. The intervention group (n = 873) was offered a comprehensive, integrated, and tightly managed system of care coordination, disease management, and preventive services provided by community-based nurse care managers working collaboratively with primary care providers. The control group (n = 863) received usual care. Overall, a 25% lower relative risk of death (hazard ratio [HR] 0.75 [95% CI 0.57-1.00], p = 0.047) was observed among intervention participants with 86 (9.9%) deaths in the intervention group and 111 (12.9%) deaths in the control group during a mean follow-up of 4.2 years. When covariates for sex, age group, primary diagnosis, perceived health, number of medications taken, hospital stays in the past 6 months, and tobacco use were included, the adjusted HR was 0.73 (95% CI 0.55-0.98, p = 0.033). Subgroup analyses did not demonstrate statistically significant interaction effects for any subgroup. No suspected program-related adverse events were identified.
Conclusions: The HQP model of community-based nurse care management appeared to reduce all-cause mortality in chronically ill older adults. Limitations of the study are that few low-income and non-white individuals were enrolled and implementation was in a single geographic region of the US. Additional research to confirm these findings and determine the model's scalability and generalizability is warranted.
Trial registration: ClinicalTrials.gov NCT01071967. Please see later in the article for the Editors' Summary.
Conflict of interest statement
All authors are paid employees of Health Quality Partners, a nonprofit health care quality research and development organization.
Figures
Comment in
-
Averting an impending storm: can we reengineer health systems to meet the needs of aging populations?PLoS Med. 2012;9(7):e1001267. doi: 10.1371/journal.pmed.1001267. Epub 2012 Jul 17. PLoS Med. 2012. PMID: 22815655 Free PMC article.
References
-
- Pham HH, Schrag D, O'Malley AS, Wu B, Bach PB. Care patterns in medicare and their implications for pay for performance. N Engl J Med. 2007;356:1130–1139. - PubMed
-
- Jencks SF, Williams MV, Coleman EA. Rehospitalizations among patients in the Medicare fee-for-service program. N Engl J Med. 2009;360:1418–1428. - PubMed
-
- McGlynn EA, Asch SM, Adams J, Keesey J, Hicks J, et al. The quality of health care delivered to adults in the United States. N Engl J Med. 2003;348:2635–2645. - PubMed
-
- CBO. High-cost medicare beneficiaries. Washington (D.C.): US Congressional Budget Office Paper; 2005. Available: http://www.cbo.gov/publication/16487. Accessed 06/06/2012.
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
