

Comparing Costs of Telephone vs Face-to-Face Extended-Care Programs for the Management of Obesity in Rural Settings
- PMID: 22818246
- PMCID: PMC3432696
- DOI: 10.1016/j.jand.2012.05.002
Comparing Costs of Telephone vs Face-to-Face Extended-Care Programs for the Management of Obesity in Rural Settings
Abstract
Background: A major challenge after successful weight loss is continuing the behaviors required for long-term weight maintenance. This challenge can be exacerbated in rural areas with limited local support resources.
Objective: This study describes and compares program costs and cost effectiveness for 12-month extended-care lifestyle maintenance programs after an initial 6-month weight-loss program.
Design: We conducted a 1-year prospective randomized controlled clinical trial.
Participants/setting: The study included 215 female participants age 50 years or older from rural areas who completed an initial 6-month lifestyle program for weight loss. The study was conducted from June 1, 2003 to May 31, 2007.
Intervention: The intervention was delivered through local Cooperative Extension Service offices in rural Florida. Participants were randomly assigned to a 12-month extended-care program using either individual telephone counseling (n=67), group face-to-face counseling (n=74), or a mail/control group (n=74).
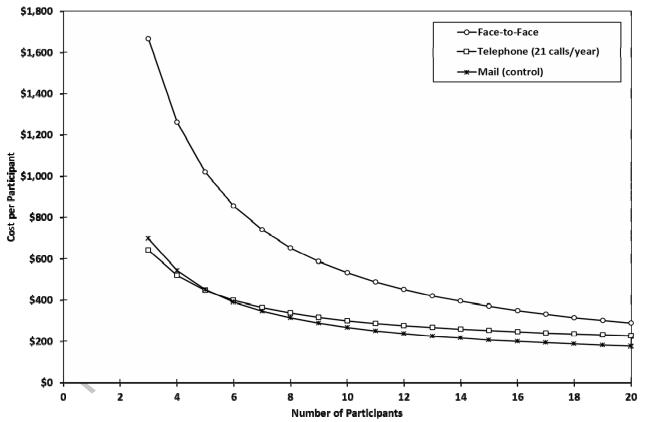
Main outcome measures: Program delivery costs, weight loss, and self-reported health status were directly assessed through questionnaires and program activity logs. Costs were estimated across a range of enrollment sizes to allow inferences beyond the study sample.
Statistical analyses performed: Nonparametric and parametric tests of differences across groups for program outcomes were combined with direct program cost estimates and expected value calculations to determine which scales of operation favored alternative formats for lifestyle maintenance.
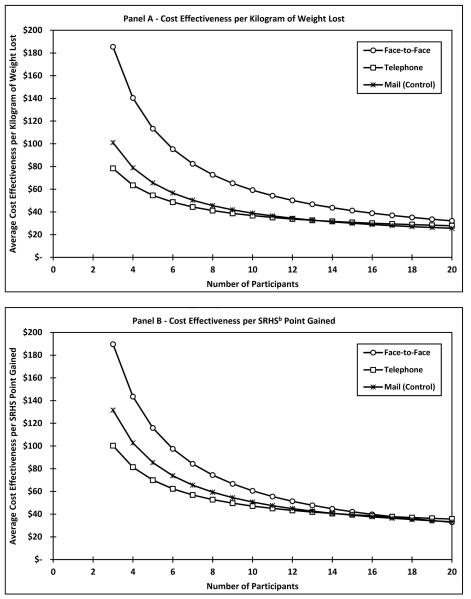
Results: Median weight regain during the intervention year was 1.7 kg for participants in the face-to-face format, 2.1 kg for the telephone format, and 3.1 kg for the mail/control format. For a typical group size of 13 participants, the face-to-face format had higher fixed costs, which translated into higher overall program costs ($420 per participant) when compared with individual telephone counseling ($268 per participant) and control ($226 per participant) programs. Although the net weight lost after the 12-month maintenance program was higher for the face-to-face and telephone programs compared with the control group, the average cost per expected kilogram of weight lost was higher for the face-to-face program ($47/kg) compared with the other two programs (approximately $33/kg for telephone and control).
Conclusions: Both the scale of operations and local demand for programs are important considerations in selecting a delivery format for lifestyle maintenance. In this study, the telephone format had a lower cost but similar outcomes compared with the face-to-face format.
Copyright © 2012 Academy of Nutrition and Dietetics. Published by Elsevier Inc. All rights reserved.
Figures
References
-
- Eberhardt MS, Ingram DD, Makuc DM, et al. Urban and rural health chartbook: Health United States, 2001. National Center for Health Statistics; Hyattsville, MD: 2001.
-
- Jackson JE, Doescher MP, Jerant AF, Hart LG. A national study of obesity prevalence and trends by type of rural county. J Rural Health. 2005;21(2):140–148. - PubMed
-
- Lutfiyya MN, Lipsky MS, Wisdom-Behounek J, Inpanbutr-Martinkus M. Is rural residency a risk factor for overweight and obesity for US children? Obesity. 2007;15(9):2348–2356. Silver Spring. - PubMed
-
- Patterson PD, Moore CG, Probst JC, Shinogle JA. Obesity and physical inactivity in rural America. J Rural Health. 2004;20(2):151–159. - PubMed
-
- Call KT, Casey MM, Radcliff T. Rural beneficiaries with chronic conditions: Does prevalence pose a risk to medicare managed care? Managed Care Quarterly. 2000;8(3):48–57. - PubMed
