

Therapeutic efficacy and safety of dihydroartemisinin-piperaquine versus artesunate-mefloquine in uncomplicated Plasmodium falciparum malaria in India
- PMID: 22818552
- PMCID: PMC3424202
- DOI: 10.1186/1475-2875-11-233
Therapeutic efficacy and safety of dihydroartemisinin-piperaquine versus artesunate-mefloquine in uncomplicated Plasmodium falciparum malaria in India
Abstract
Background: Resistance in Plasmodium falciparum to commonly used anti-malarial drugs, especially chloroquine, is being increasingly documented in India. By 2007, the first-line treatment for uncomplicated malaria has been revised to recommend artemisinin-based combination therapy (ACT) for all confirmed P. falciparum cases.
Objective: The objective of this study was to compare the efficacy, safety and tolerability between dihydroartemisinin-piperaquine (DP) and artesunate plus mefloquine (A + M) drug combinations in the treatment of uncomplicated P. falciparum malaria in India.
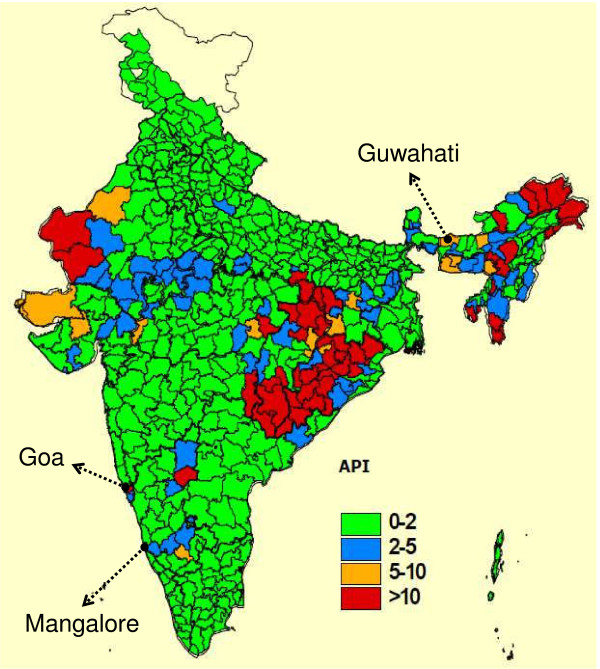
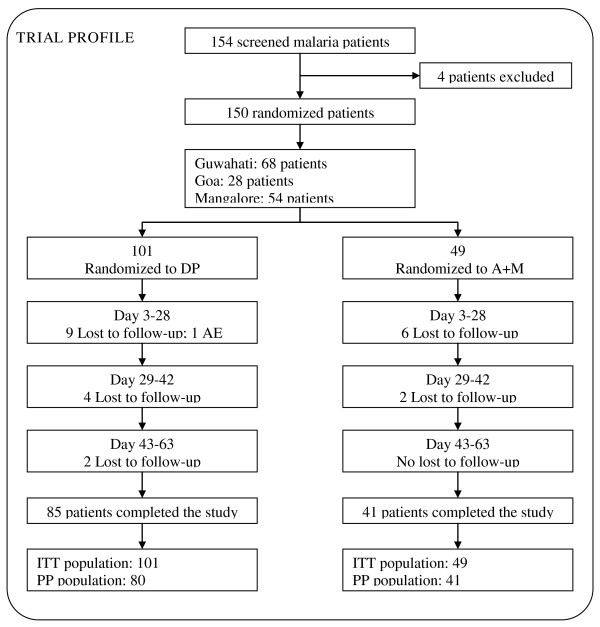
Methods: Between 2006 and 2007, 150 patients with acute uncomplicated P. falciparum malaria were enrolled, randomized to DP (101) or A + M (49) and followed up for 63 days as part of an open-label, non-inferiority, randomized, phase III multicenter trial in Asia.
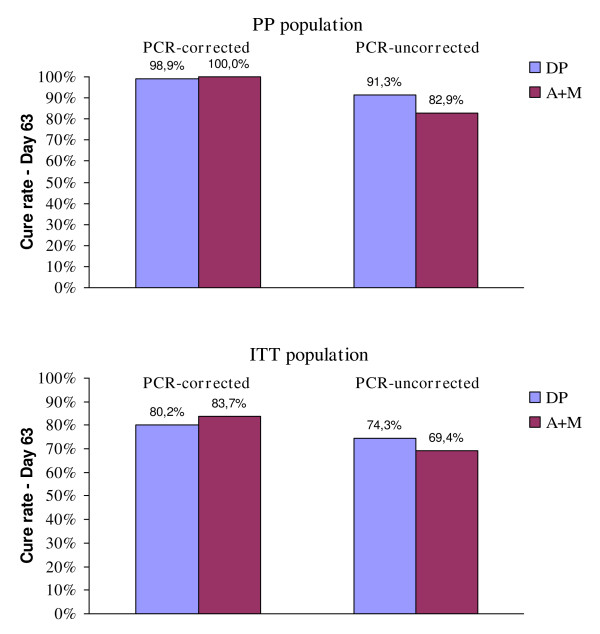
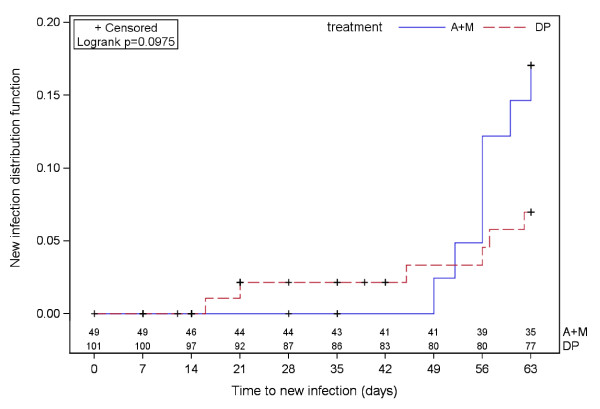
Results: The heterogeneity analysis showed no statistically significant difference between India and the other countries involved in the phase III study, for both the PCR-corrected and uncorrected cure rates. As shown at the whole study level, both forms of ACT were highly efficacious in India. In fact, in the per protocol population, the 63-day cure rates were 100% for A + M and 98.8% for DP. The DP combination exerted a significant post-treatment prophylactic effect, and compared with A + M a significant reduction in the incidence of new infections for DP was observed (respectively 17.1% versus 7.5% of patients experienced new infection within follow up). Parasite and fever clearance was rapid in both treatment arms (median time to parasite clearance of one day for both groups). Both DP and A + M were well tolerated, with the majority of adverse events of mild or moderate severity. The frequencies of individual adverse events were generally similar between treatments, although the incidence of post treatment adverse events was slightly higher in patients who received A + M with respect to those treated with DP.
Conclusion: DP is a new ACT displaying high efficacy and safety in the treatment of uncomplicated P. falciparum malaria and could potentially be considered for the first-line treatment of uncomplicated falciparum malaria in India.
Trial registration: Current Controlled Trials ISRCTN 81306618.
Figures
References
-
- Jain S, Chugh TD. An overview of malaria burden in India and road-blocks in its control. J Clin Diagnostic Res. 2011;5:915–916.
-
- Kumar A, Valecha N, Jain T, Dash AP. Burden of malaria in India: retrospective and prospective view. AmJ Trop Med Hyg. 2007;77:69–78. - PubMed
-
- Tyagi P, Roy A, Malhotra MS. Knowledge, awareness and practices towards malaria in communities of rural, semi-rural and bordering areas of east Delhi India. J Vect Borne Dis. 2005;42:30–35. - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Research Materials
