

Ultrasonographic quantification of spinal cord and dural pulsations during cervical laminoplasty in patients with compressive myelopathy
- PMID: 22820915
- PMCID: PMC3508211
- DOI: 10.1007/s00586-012-2430-9
Ultrasonographic quantification of spinal cord and dural pulsations during cervical laminoplasty in patients with compressive myelopathy
Abstract
Purpose: Pulsatile movements of the dura mater have been interpreted as a sign that the cord is free within the subarachnoid space, with no extrinsic compression. However, the association between restoration of pulsation and adequate decompression of the spinal cord has not been established. The present study investigated the relationship between the extent of spinal cord decompression and spinal cord and dural pulsations based on quantitative analysis of intraoperative ultrasonography (US).
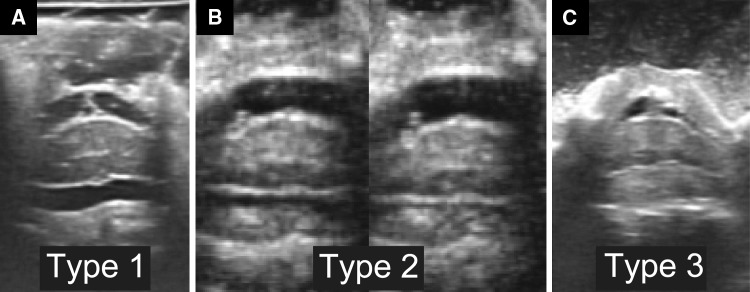
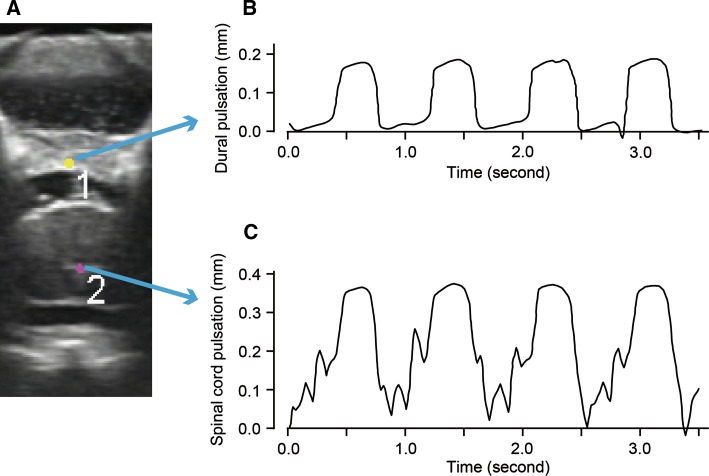
Methods: Eighty-five consecutive patients (55 males, 30 females; mean age, 64 ± 13 years) who underwent cervical double-door laminoplasty to relieve compressive myelopathy were enrolled. Spinal cord decompression status was classified as: Type 1 (non-contact), the subarachnoid space was retained on the ventral side of the cord, Type 2 (contact and apart), the cord showed both contact with and separation from the anterior element of the cervical spine, or Type 3 (contact), the cord showed continuous contact with the anterior element of the cervical spine. Spinal cord and dura mater dynamics were quantitatively analyzed using automatic video-tracking software. Furthermore, the intensity of spinal and dural pulsation was compared with the recovery of motor function at 1 year after surgery as measured by increase in the Japanese Orthopaedic Association Cervical Myelopathy Evaluation Questionnaire (JOACMEQ).
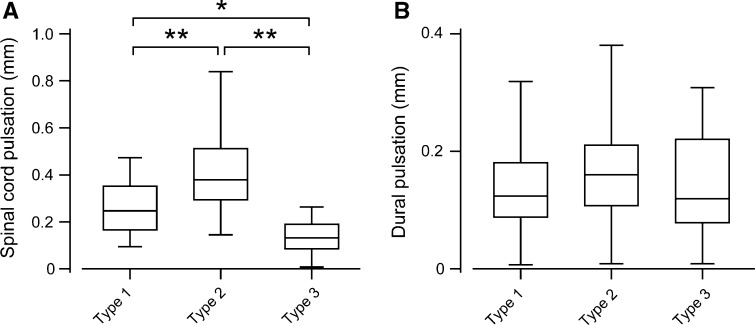
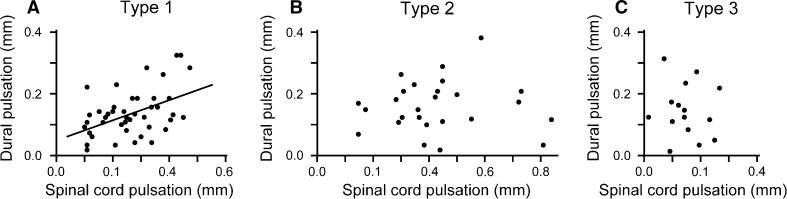
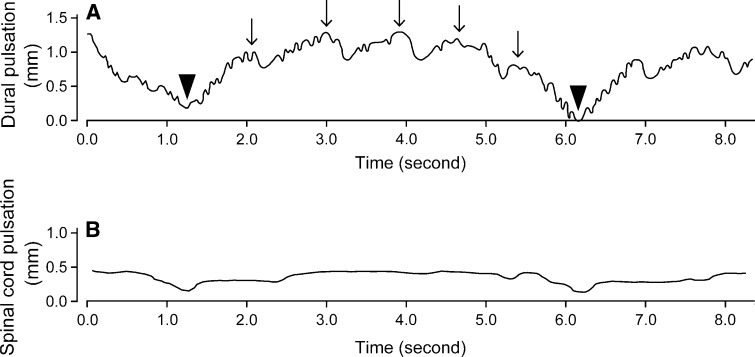
Results: Spinal cord pulsation amplitude ranged from 0.01 to 0.84 mm (mean 0.30 ± 0.16 mm) and dural pulsation amplitude ranged from 0.01 to 0.38 mm (mean 0.14 ± 0.08 mm). Average spinal cord pulsation amplitude in Type 2 patients was significantly larger than that in the other groups, whereas, average dural pulsation amplitudes were similar for all three groups. There was a significant correlation between spinal cord and dural pulsation amplitudes in Type 1 patients, but not in Type 2 or Type 3 patients. Type 3 patients showed a particularly poor correlation between spinal cord and dural pulsations. Spinal cord pulsation amplitude was moderately correlated with the recovery of motor function evaluated by JOACMEQ.
Conclusion: The present results suggest that restoration of dural pulsation is not an adequate indicator of sufficient decompression of the spinal cord following a surgical procedure.
Figures
References
-
- Enzmann DR, Pelc NJ. Normal flow patterns of intracranial and spinal cerebrospinal fluid defined with phase-contrast cine MR imaging. Radiology. 1991;178:467–474. - PubMed
-
- Fukui M, Chiba K, Kawakami M, Kikuchi S, Konno S, Miyamoto M, Seichi A, Shimamura T, Shirado O, Taguchi T, Takahashi K, Takeshita K, Tani T, Toyama Y, Yonenobu K, Wada E, Tanaka T, Hirota Y. JOA back pain evaluation questionnaire (JOABPEQ)/JOA cervical myelopathy evaluation questionnaire (JOACMEQ). The report on the development of revised versions. April 16, 2007. The subcommittee of the clinical outcome committee of the japanese orthopaedic association on low back pain and cervical myelopathy evaluation. J Orthop Sci. 2009;14:348–365. doi: 10.1007/s00776-009-1337-8. - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
