

Association between maternal age and birth defects of unknown etiology: United States, 1997-2007
- PMID: 22821755
- PMCID: PMC4532312
- DOI: 10.1002/bdra.23049
Association between maternal age and birth defects of unknown etiology: United States, 1997-2007
Abstract
Background: Birth defects affect 3% of babies born, and are one of the leading causes of infant mortality. Both younger and older maternal age may pose increased risks for certain birth defects. This study assessed the relationship between maternal age at the estimated delivery date and the risk for birth defects.
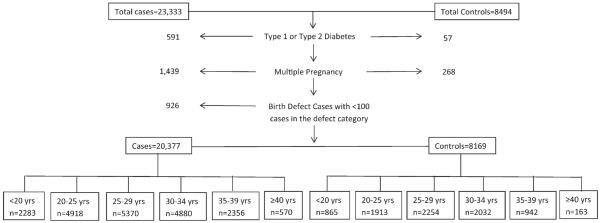
Methods: Data were obtained from the National Birth Defects Prevention Study, a population-based case-control study including mothers across 10 states. Maternal age was stratified into six categories: <20, 20 to 24, 25 to 29, 30 to 34, 35 to 39, and ≥40 years, and also analyzed as a continuous variable. Logistic regression models adjusted formaternal race/ethnicity, education, body mass index (BMI), folic acid use, smoking, gravidity, and parental age difference were used to estimate adjusted odds ratios (aORs) and 95% confidence intervals (CIs).
Results: For maternal age <20 years, associations with total anomalous pulmonary venous return (aOR, 2.3; 95% CI, 1.3-4.0), amniotic band sequence (aOR, 2.4; 95% CI, 1.5-3.8), and gastroschisis (aOR, 6.1; 95% CI, 4.8-8.0) were observed. For the ≥40 year age group, associations with several cardiac defects, esophageal atresia (aOR, 2.9; 95% CI, 1.7-4.9), hypospadias (aOR, 2.0; 95% CI, 1.4-3.0), and craniosynostosis (aOR, 1.6; 95% CI, 1.1-2.4) were observed. Results using maternal age as a continuous variable were consistent with those that used categorized maternal age.
Conclusion: Elucidating risk factors specific to women ateither extreme of maternal age may offer prevention opportunities. All women should be made aware of prevention opportunities, such as folic acid supplementation, to reduce the occurrence of birth defects.
Copyright © 2012 Wiley Periodicals, Inc.
Figures
Similar articles
-
Associations between maternal periconceptional exposure to secondhand tobacco smoke and major birth defects.Am J Obstet Gynecol. 2016 Nov;215(5):613.e1-613.e11. doi: 10.1016/j.ajog.2016.07.022. Epub 2016 Jul 18. Am J Obstet Gynecol. 2016. PMID: 27443814
-
Maternal injuries during the periconceptional period and the risk of birth defects, National Birth Defects Prevention Study, 1997-2005.Paediatr Perinat Epidemiol. 2011 Sep;25(5):487-96. doi: 10.1111/j.1365-3016.2011.01215.x. Epub 2011 Jul 21. Paediatr Perinat Epidemiol. 2011. PMID: 21819430
-
Specific birth defects in pregnancies of women with diabetes: National Birth Defects Prevention Study, 1997-2011.Am J Obstet Gynecol. 2020 Feb;222(2):176.e1-176.e11. doi: 10.1016/j.ajog.2019.08.028. Epub 2019 Aug 24. Am J Obstet Gynecol. 2020. PMID: 31454511 Free PMC article.
-
Comparative analysis of perinatal outcomes and birth defects amongst adolescent and older Ugandan mothers: evidence from a hospital-based surveillance database.Reprod Health. 2021 Mar 4;18(1):56. doi: 10.1186/s12978-021-01115-w. Reprod Health. 2021. PMID: 33663555 Free PMC article.
-
Folic acid supplementation and malaria susceptibility and severity among people taking antifolate antimalarial drugs in endemic areas.Cochrane Database Syst Rev. 2022 Feb 1;2(2022):CD014217. doi: 10.1002/14651858.CD014217. Cochrane Database Syst Rev. 2022. PMID: 36321557 Free PMC article.
Cited by
-
The Differences of Population Birth Defects in Epidemiology Analysis between the Rural and Urban Areas of Hunan Province in China, 2014-2018.Biomed Res Int. 2021 Apr 21;2021:2732983. doi: 10.1155/2021/2732983. eCollection 2021. Biomed Res Int. 2021. PMID: 33969116 Free PMC article.
-
Newborn screening for sickle cell disease in Butembo and Beni: a pilot experience in a highland region of the Democratic Republic of Congo.Pan Afr Med J. 2023 May 24;45:56. doi: 10.11604/pamj.2023.45.56.36087. eCollection 2023. Pan Afr Med J. 2023. PMID: 37637401 Free PMC article.
-
Frequency of Congenital Anomalies in the Brazilian Midwest and the Association with Maternal Risk Factors: Case-control Study.Rev Bras Ginecol Obstet. 2020 Apr;42(4):188-193. doi: 10.1055/s-0040-1709692. Epub 2020 Apr 24. Rev Bras Ginecol Obstet. 2020. PMID: 32330960 Free PMC article.
-
Trends in the prevalences of congenital anomalies and age at motherhood in a Southern European region: a population-based study.BMJ Open. 2014 Mar 3;4(3):e004244. doi: 10.1136/bmjopen-2013-004244. BMJ Open. 2014. PMID: 24589823 Free PMC article.
-
Detection of Zika virus infection among asymptomatic pregnant women in the North of Peru.BMC Res Notes. 2018 May 18;11(1):311. doi: 10.1186/s13104-018-3400-z. BMC Res Notes. 2018. PMID: 29776426 Free PMC article.
References
-
- American Society for Reproductive Medicine (ASRM) Age and fertility: a guide for patients. 2003.
-
- Baird PA, Sadovnick AD, Yee IM. Maternal age and birth defects: a population study. Lancet. 1991;337:527–530. - PubMed
-
- Benjamin BG, Ethen MK, Van Hook CL, et al. Gastroschisis prevalence in Texas 1999–2003. Birth Defects Res A Clin Mol Teratol. 2010;88:178–185. - PubMed
-
- Bower C, Norwood F, Knowles S, et al. Amniotic band syndrome: a population-based study in two Australian states. Paediatr Perinat Epidemiol. 1993;7:395–403. - PubMed
-
- Brent RL. Utilization of developmental basic science principles in the evaluation of reproductive risks from pre- and postconception environmental radiation exposures. Teratology. 1999;59:182–204. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
