

The effect of intraoperative infusion of dexmedetomidine on the quality of recovery after major spinal surgery
- PMID: 22824921
- PMCID: PMC3557800
- DOI: 10.1097/ANA.0b013e31826318af
The effect of intraoperative infusion of dexmedetomidine on the quality of recovery after major spinal surgery
Abstract
Background: Surgery induces a variety of metabolic, endocrine, and immune changes collectively known as the "stress response," which may often lead to prolonged postoperative convalescence. Anesthetic management may modulate this physiological response, thus affecting the postoperative course. We hypothesized that the intraoperative administration of dexmedetomidine (DEX), a sympatholytic agent, would reduce the stress response and improve the quality of recovery in patients undergoing major surgery.
Methods: We conducted a prospective randomized double-blinded study of 54 patients undergoing multilevel spinal fusion. Anesthesia was maintained using either propofol/fentanyl/dexmedetomidine (PFD) or propofol/fentanyl/placebo-saline (PFS). The quality of recovery (a primary endpoint) was assessed using a 40-item quality of recovery questionnaire and a 9-question Fatigue Severity Scores. The tests were carried out preoperatively on postoperative days (POD) 1, 2, 3, and 30. Blood samples were collected at baseline, in the postanesthesia care unit, and at POD 1 and were analyzed for levels of cortisol, C-reactive proteins (CRP), and cytokines interleukin (IL)-1α, IL-1β, IL-1ra, IL-2, IL-6, IL-8, IL-10, and tumor necrosis factor-α. Data were analyzed using SPSS software (version 18) using a multivariate and mixed model approach to test for the effect of surgery and drug group. Pairwise comparisons were assessed by means of the t test or rank tests after correcting for multiple comparisons.
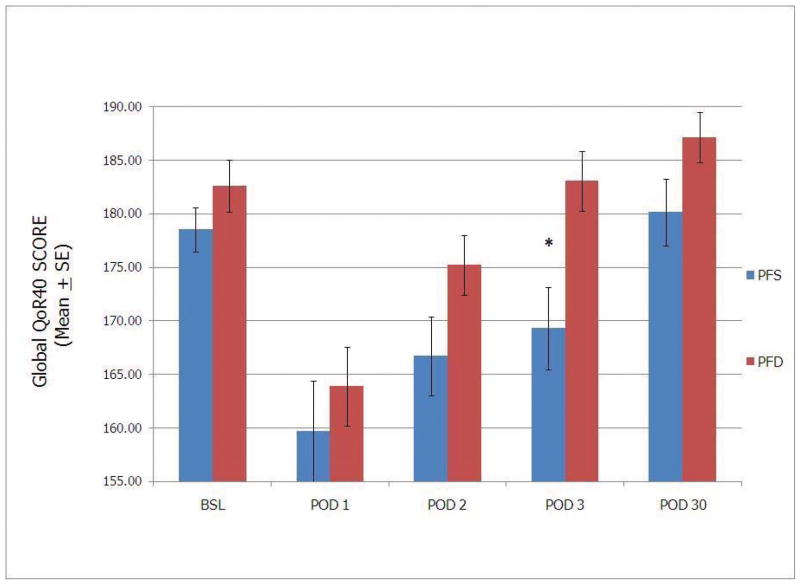
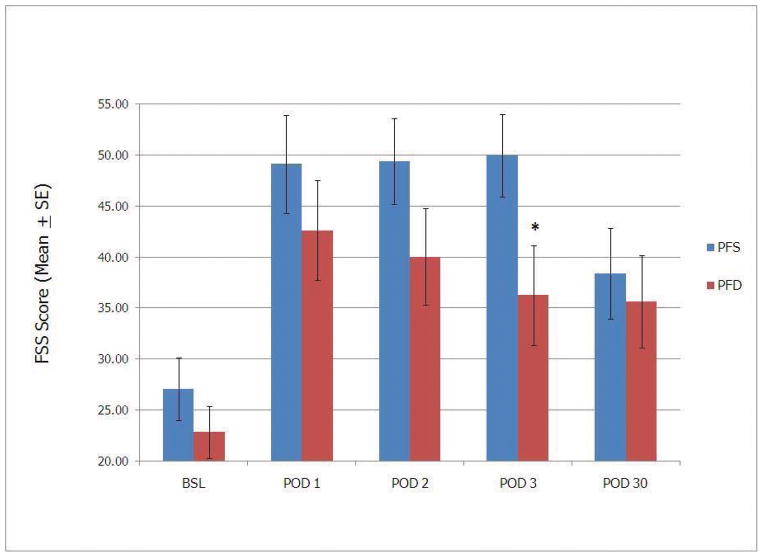
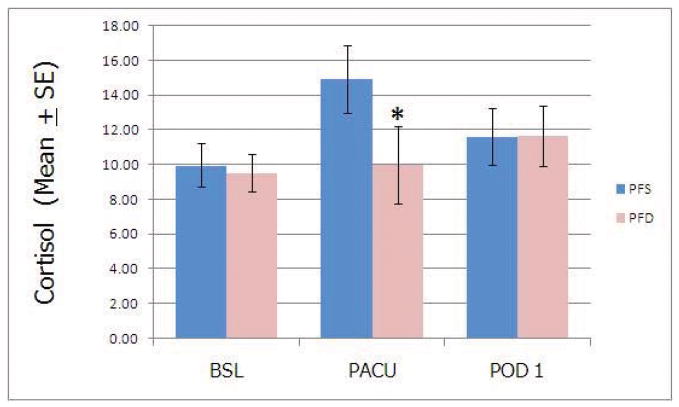
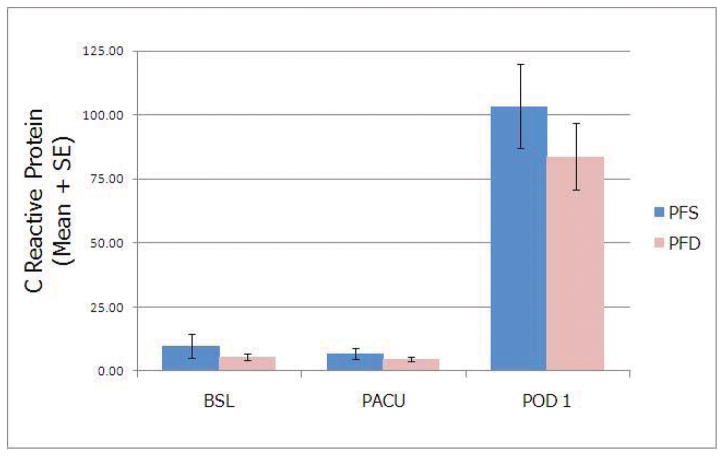
Results: The global 40-item quality of recovery questionnaire scores showed a significant effect of time (F(4,114)=22.63, P<0.001) and drug (F(1,51)=4.368, P=0.042), with average scores decreasing to lower values on POD 1 (163.63±2.47) and POD 2 (170.94±2.38) compared with baseline (180.56±1.588, mean±SE, 2-tailed t tests, P<0.001). By POD 3, scores were significantly lower (-13.74 point difference, P=0.005) in the PFS group (169.3±3.87) than in the PFD group (183.04±2.76). All patients reported significantly higher levels of fatigue postoperatively, but intergroup difference in Fatigue Severity Scores was detected on POD 3 only, with scores in the PFS group higher than in the PFD group (50.0±4.0 vs. 36.3±4.9, P=0.035). In both groups, plasma cortisol levels were highest in the postanesthesia care unit, whereas CRP levels were elevated on POD 1. DEX significantly reduced the levels of cortisol, but not those of CRP. Levels of cytokines IL-6, IL-8, and IL-10 were significantly higher immediately after surgery and at POD 1. Plasma levels of other cytokines were not affected by surgery. DEX delayed postoperative rise in IL-10 but not in IL-6 or IL-8.
Conclusions: DEX infusion during multilevel spinal fusions moderately improved the quality of recovery and possibly reduced fatigue in the early postoperative period. Moreover, it reduced plasma levels of cortisol and IL-10 in comparison with the control group. Our sample size was not sufficient to detect differences either in the incidence of complications or in clinically relevant outcomes.
Conflict of interest statement
Conflicts: Alex Bekker received honoraria for presentations (in the past) and research funding from Hospira
Figures
Comment in
-
Does the detailed formula of propofol matter in studies focusing on inflammatory response?J Neurosurg Anesthesiol. 2013 Apr;25(2):208-9. doi: 10.1097/ANA.0b013e31828676ed. J Neurosurg Anesthesiol. 2013. PMID: 23434752 No abstract available.
-
In reply.J Neurosurg Anesthesiol. 2013 Apr;25(2):209. doi: 10.1097/01.ana.0000428055.36003.6e. J Neurosurg Anesthesiol. 2013. PMID: 23434753 No abstract available.
References
-
- Homburger JA, Meiler SE. Anesthesia drugs, immunity, and long-term outcome. Curr Opin Anaesthesiol. 2006;19:423–8. - PubMed
-
- Kurosawa S, Kato M. Anesthetics, immune cells, and immune responses. J Anesth. 2008;22:263–77. - PubMed
-
- Kennedy BC, Hall GM. Neuroendocrine and inflammatory aspects of surgery: do they affect outcome? Acta Anaesthesiol Belg. 1999;50:205–9. - PubMed
-
- Westaby S, Saatvedt K, White S, Katsumata T, van Oeveren W, Halligan PW. Is there a relationship between cognitive dysfunction and systemic inflammatory response after cardiopulmonary bypass? Ann Thorac Surg. 2001;71:667–72. - PubMed
-
- Goldfarb Y, Sorski L, Benish M, Levi B, Melamed R, Ben-Eliyahu S. Improving postoperative immune status and resistance to cancer metastasis: a combined perioperative approach of immunostimulation and prevention of excessive surgical stress responses. Ann Surg. 2011;253:798–810. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
