

A method for estimating zero-flow pressure and intracranial pressure
- PMID: 22824923
- PMCID: PMC3524356
- DOI: 10.1097/ANA.0b013e318263c295
A method for estimating zero-flow pressure and intracranial pressure
Abstract
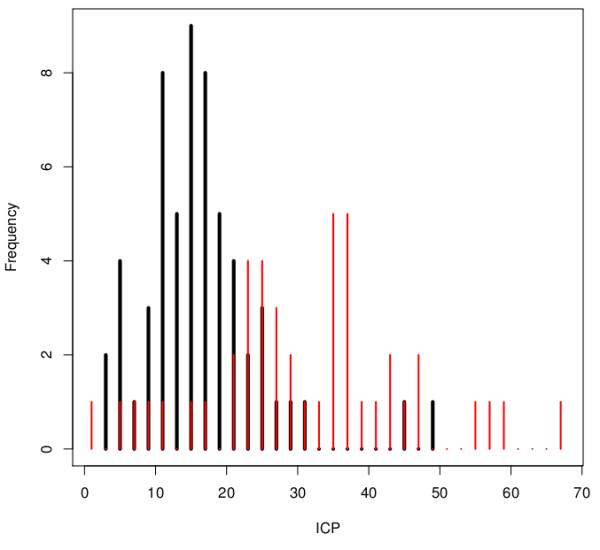
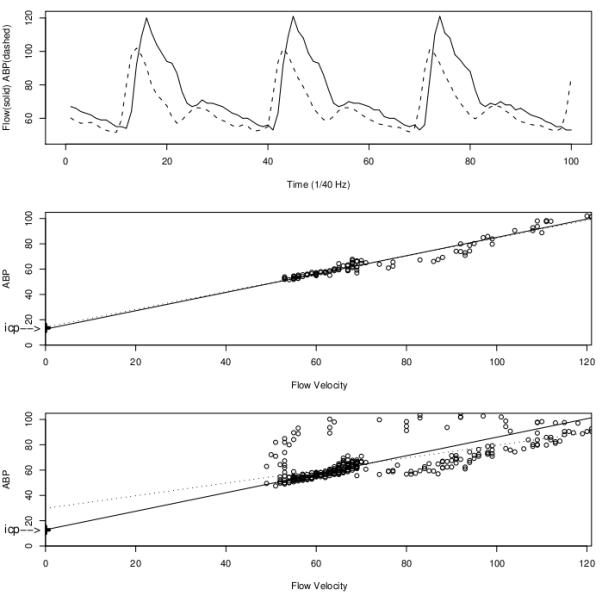
Background: It has been hypothesized that the critical closing pressure of cerebral circulation, or zero-flow pressure (ZFP), can estimate intracranial pressure (ICP). One ZFP estimation method used extrapolation of arterial blood pressure as against blood-flow velocity. The aim of this study was to improve ICP predictions.
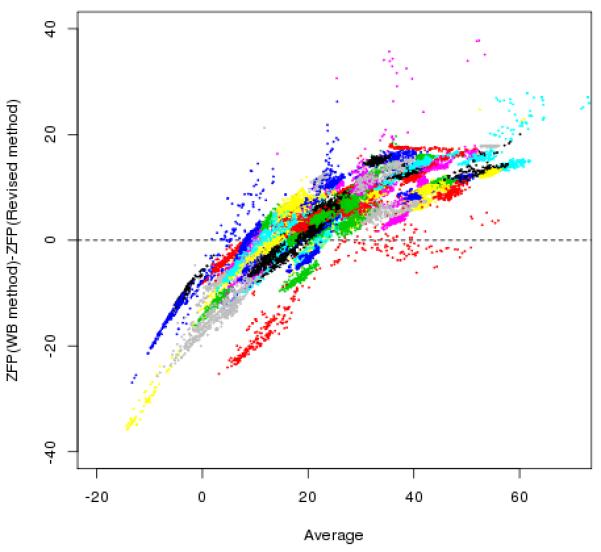
Methods: Two revisions have been considered: (1) the linear model used for extrapolation is extended to a nonlinear equation; and (2) the parameters of the model are estimated by an alternative criterion (not least squares). The method is applied to data on transcranial Doppler measurements of blood-flow velocity, arterial blood pressure, and ICP from 104 patients suffering from closed traumatic brain injury, sampled across the United States and England.
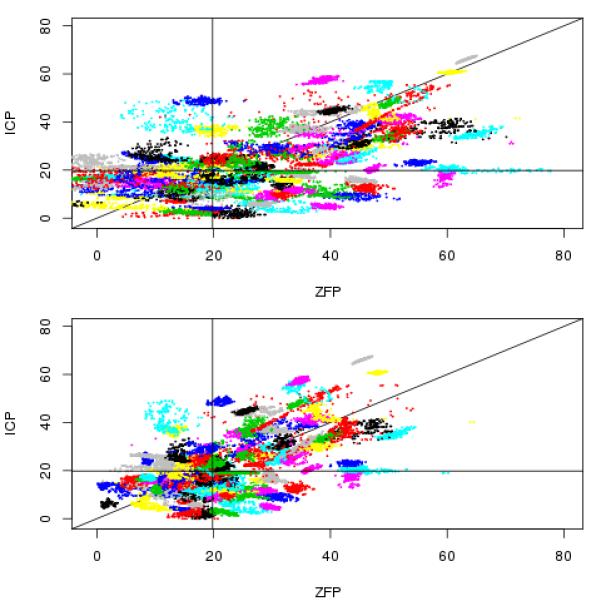
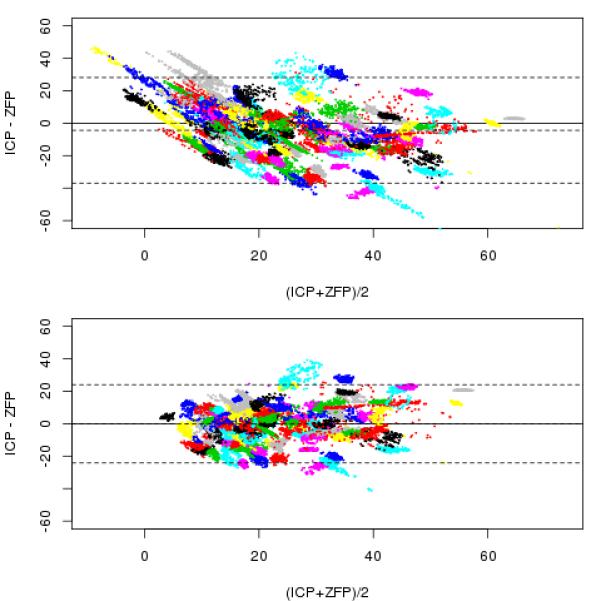
Results: The revisions lead to qualitative (eg, precluding negative ICP) and quantitative improvements in ICP prediction. While moving from the original to the revised method, the ±2 SD of the error is reduced from 33 to 24 mm Hg, and the root-mean-squared error is reduced from 11 to 8.2 mm Hg. The distribution of root-mean-squared error is tighter as well; for the revised method the 25th and 75th percentiles are 4.1 and 13.7 mm Hg, respectively, as compared with 5.1 and 18.8 mm Hg for the original method.
Conclusions: Proposed alterations to a procedure for estimating ZFP lead to more accurate and more precise estimates of ICP, thereby offering improved means of estimating it noninvasively. The quality of the estimates is inadequate for many applications, but further work is proposed, which may lead to clinically useful results.
Figures
Similar articles
-
Extrapolation to zero-flow pressure in cerebral arteries to estimate intracranial pressure.Br J Anaesth. 2003 Mar;90(3):291-5. doi: 10.1093/bja/aeg073. Br J Anaesth. 2003. PMID: 12594138
-
Comparison of Different Calibration Methods in a Non-invasive ICP Assessment Model.Acta Neurochir Suppl. 2018;126:79-84. doi: 10.1007/978-3-319-65798-1_17. Acta Neurochir Suppl. 2018. PMID: 29492537
-
Cerebral Critical Closing Pressure: Is the Multiparameter Model Better Suited to Estimate Physiology of Cerebral Hemodynamics?Neurocrit Care. 2016 Dec;25(3):446-454. doi: 10.1007/s12028-016-0288-0. Neurocrit Care. 2016. PMID: 27389005
-
Critical closing pressure during intracranial pressure plateau waves.Neurocrit Care. 2013 Jun;18(3):341-8. doi: 10.1007/s12028-013-9830-5. Neurocrit Care. 2013. PMID: 23512327
-
Transcranial Doppler measurements.New Horiz. 1995 Aug;3(3):423-30. New Horiz. 1995. PMID: 7496750 Review.
Cited by
-
The method described by Czosnyka is particularly suitable for measuring CPPe in patients undergoing cerebral angiography.Front Surg. 2025 Jan 6;11:1488265. doi: 10.3389/fsurg.2024.1488265. eCollection 2024. Front Surg. 2025. PMID: 39834503 Free PMC article.
References
-
- Becker D, et al. The outcome from severe head injury with early diagnosis and intensive management. J Neurosurg. 1977;47:491–502. - PubMed
-
- Miller J, et al. Further experience in the management of severe head injury. J Neurosurg. 1981;54:289–99. - PubMed
-
- Narayan R, et al. Improved confidence of outcome prediction in severe head injury. A comparative analysis of the clinical examination, multimodality evoked potentials, CT scanning, and intracranial pressure. J Neurosurg. 1981;54:751–62. - PubMed
-
- Narayan R, et al. Intracranial pressure: to monitor or not to monitor? A review of our experience with head injury. J Neurosurg. 1982;56:650–659. - PubMed
-
- Saul T, Ducker T. Effect of intracranial pressure monitoring and aggressive treatment on mortality in severe head injury. J Neurosurg. 1982;56:498–503. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
