

Fluid balance in critically ill children with acute lung injury
- PMID: 22824936
- PMCID: PMC3455114
- DOI: 10.1097/CCM.0b013e31825bc54d
Fluid balance in critically ill children with acute lung injury
Abstract
Objectives: In the Fluid and Catheter Treatment Trial (NCT00281268), adults with acute lung injury randomized to a conservative vs. liberal fluid management protocol had increased days alive and free of mechanical ventilator support (ventilator-free days). Recruiting sufficient children with acute lung injury into a pediatric trial is challenging. A Bayesian statistical approach relies on the adult trial for the a priori effect estimate, requiring fewer patients. Preparing for a Bayesian pediatric trial mirroring the Fluid and Catheter Treatment Trial, we aimed to: 1) identify an inverse association between fluid balance and ventilator-free days; and 2) determine if fluid balance over time is more similar to adults in the Fluid and Catheter Treatment Trial liberal or conservative arms.
Design: Multicentered retrospective cohort study.
Setting: Five pediatric intensive care units.
Patients: Mechanically ventilated children (age≥1 month to <18 yrs) with acute lung injury admitted in 2007-2010.
Interventions: None.
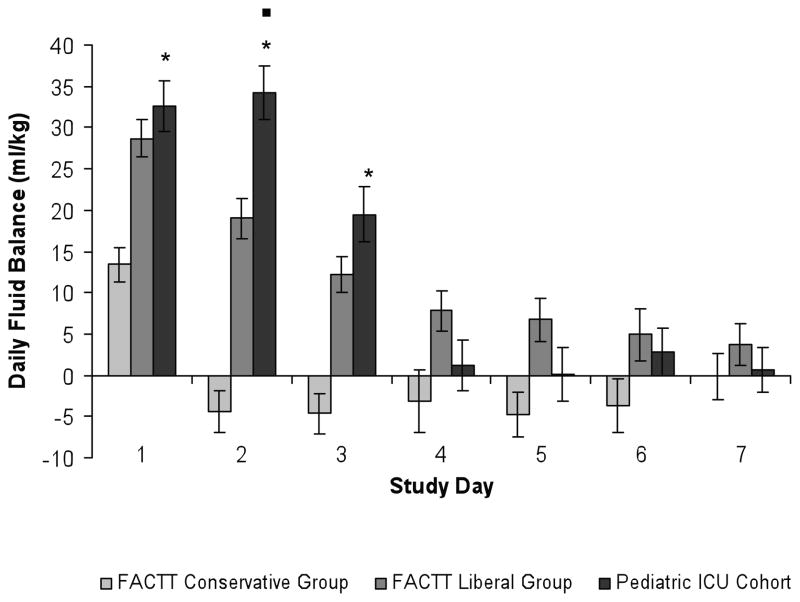
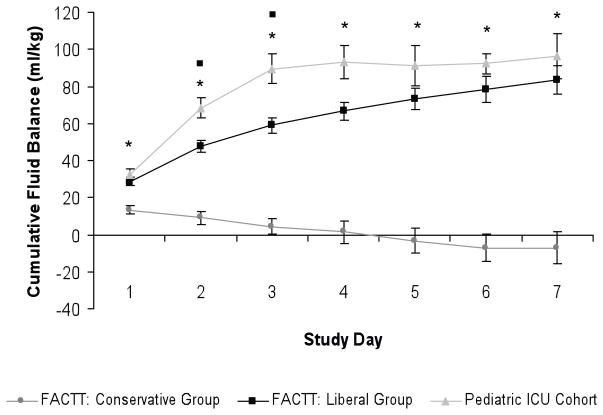
Measurements and main results: Fluid intake, output, and net fluid balance were collected on days 1-7 in 168 children with acute lung injury (median age 3 yrs, median PaO2/FIO2 138) and weight-adjusted (mL/kg). Using multivariable linear regression to adjust for age, gender, race, admission day illness severity, PaO2/FIO2, and vasopressor use, increasing cumulative fluid balance (mL/kg) on day 3 was associated with fewer ventilator-free days (p=.02). Adjusted for weight, daily fluid balance on days 1-3 and cumulative fluid balance on days 1-7 were higher in these children compared to adults in the Fluid and Catheter Treatment Trial conservative arm (p<.001, each day) and was similar to adults in the liberal arm.
Conclusions: Increasing fluid balance on day 3 in children with acute lung injury at these centers is independently associated with fewer ventilator-free days. Our findings and the similarity of fluid balance patterns in our cohort to adults in the Fluid and Catheter Treatment Trial liberal arm demonstrate the need to determine whether a conservative fluid management strategy improves clinical outcomes in children with acute lung injury and support a Bayesian trial mirroring the Fluid and Catheter Treatment Trial.
Conflict of interest statement
The authors do not have any financial conflicts or ethical conflicts to disclose.
Figures
Comment in
-
On balance, are fluids a marker or a target?Crit Care Med. 2012 Oct;40(10):2918-20. doi: 10.1097/CCM.0b013e31826563b6. Crit Care Med. 2012. PMID: 22986666 No abstract available.
-
Are children similar to adults when there is fluid overload?Crit Care Med. 2013 May;41(5):e48-9. doi: 10.1097/CCM.0b013e318283c361. Crit Care Med. 2013. PMID: 23591229 No abstract available.
-
The authors reply.Crit Care Med. 2013 May;41(5):e49. doi: 10.1097/CCM.0b013e31828c253e. Crit Care Med. 2013. PMID: 23591230 No abstract available.
References
-
- Ware LB, Matthay MA. The acute respiratory distress syndrome. N Engl J Med. 2000;342:1334–1349. - PubMed
-
- Luce JM. Acute lung injury and the acute respiratory distress syndrome. Crit Care Med. 1998;26:369–376. - PubMed
-
- Ware LB. Pathophysiology of acute lung injury and the acute respiratory distress syndrome. Semin Respir Crit Care Med. 2006;27:337–349. - PubMed
-
- West JB. Invited Review: Pulmonary capillary stress failure. J Appl Physiol. 2000;89:2483–2489. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
