

Oblique paraspinal approach for thoracic disc herniations using tubular retractor with robotic holder: a technical note
- PMID: 22825631
- PMCID: PMC3508237
- DOI: 10.1007/s00586-012-2438-1
Oblique paraspinal approach for thoracic disc herniations using tubular retractor with robotic holder: a technical note
Abstract
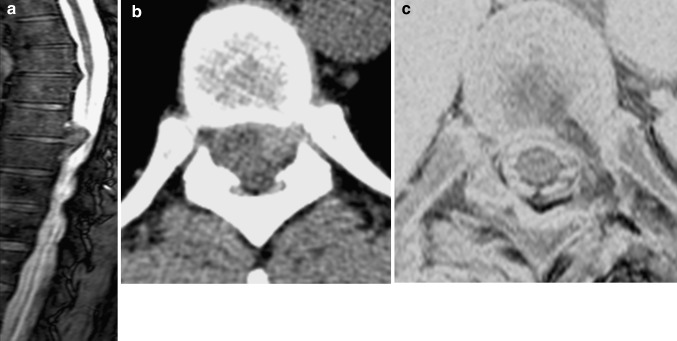
Introduction: Symptomatic thoracic disc herniations (TDHs) are uncommon and can be surgically treated. Although transthoracic decompression is considered the gold standard, it is associated with significant comorbidities. In particular, approach via a posterior laminectomy has been associated with poor results. Several strategies have been developed for the resection of TDHs without manipulating the spinal cord. We describe a minimally invasive technique by using 3-D navigation and tubular retractors with the aid of a robotic holder via an oblique paraspinal approach.
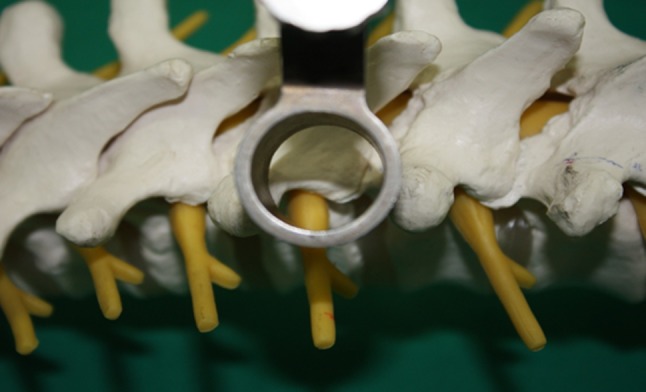
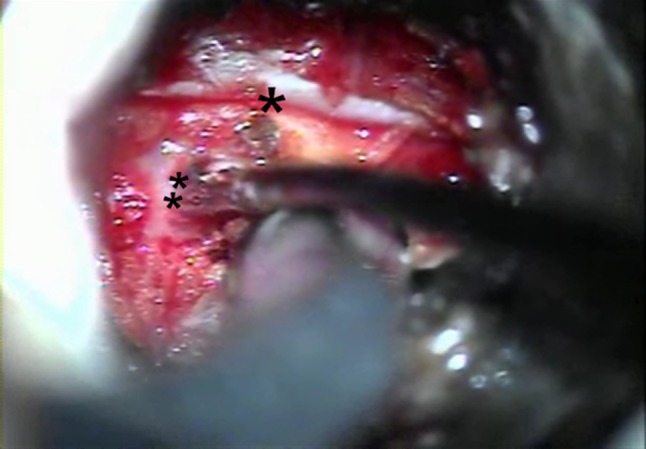
Materials and methods: The 20-mm working tube via an oblique trajectory through the fascia provides a good surgical field for thoracic discectomy through a microscope. We present our first five patients with TDHs operated using this minimally invasive approach.
Results: Neurological symptoms were improved postoperatively, and there were no surgical complications. There was no instability or recurrence during the follow-up period.
Conclusion: The oblique paraspinal approach may offer an alternative surgical option for treating TDHs.
Figures


References
-
- Benjamin V. Diagnosis and management of thoracic disc disease. Clin Neurosurg. 1983;30:577–605. - PubMed
-
- Stillerman CB, Weiss MH. Management of thoracic disc disease. Clin Neurosurg. 1992;38:325–352. - PubMed
-
- Bohlman HH, Zdeblick TA. Anterior excision of herniated thoracic discs. J Bone Joint Surg Am. 1988;70:1038–1047. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
