

Preoperative localization strategies for primary hyperparathyroidism: an economic analysis
- PMID: 22825773
- PMCID: PMC3680347
- DOI: 10.1245/s10434-012-2512-2
Preoperative localization strategies for primary hyperparathyroidism: an economic analysis
Abstract
Background: Strategies for localizing parathyroid pathology preoperatively vary in cost and accuracy. Our purpose was to compute and compare comprehensive costs associated with common localization strategies.
Methods: A decision-analytic model was developed to evaluate comprehensive, short-term costs of parathyroid localization strategies for patients with primary hyperparathyroidism. Eight strategies were compared. Probabilities of accurate localization were extracted from the literature, and costs associated with each strategy were based on 2011 Medicare reimbursement schedules. Differential cost considerations included outpatient versus inpatient surgeries, operative time, and costs of imaging. Sensitivity analyses were performed to determine effects of variability in key model parameters upon model results.
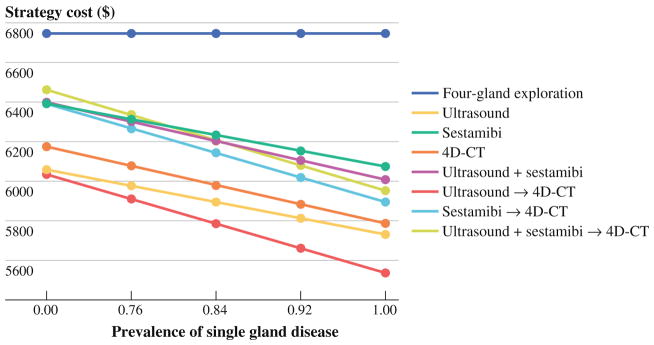
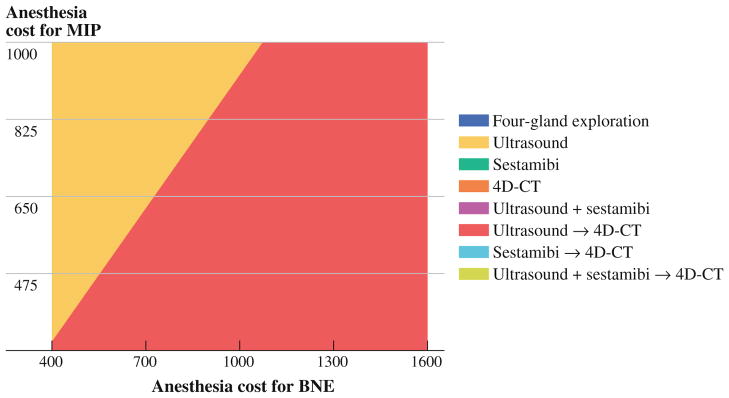
Results: Ultrasound (US) followed by 4D-CT was the least expensive strategy ($5,901), followed by US alone ($6,028), and 4D-CT alone ($6,110). Strategies including sestamibi (SM) were more expensive, with associated expenditures of up to $6,329 for contemporaneous US and SM. Four-gland, bilateral neck exploration (BNE) was the most expensive strategy ($6,824). Differences in cost were dependent upon differences in the sensitivity of each strategy for detecting single-gland disease, which determined the proportion of patients able to undergo outpatient minimally invasive parathyroidectomy. In sensitivity analysis, US alone was preferred over US followed by 4D-CT only when both the sensitivity of US alone for detecting an adenoma was ≥ 94 %, and the sensitivity of 4D-CT following negative US was ≤ 39 %. 4D-CT alone was the least costly strategy when US sensitivity was ≤ 31 %.
Conclusions: Among commonly used strategies for preoperative localization of parathyroid pathology, US followed by selective 4D-CT is the least expensive.
Figures
References
-
- The American Association of Clinical Endocrinologists and the American Association of Endocrine Surgeons position statement on the diagnosis and management of primary hyperparathyroidism. Endocr Pract. 2005;11:49–54. - PubMed
-
- Silverberg SJ, Shane E, Jacobs TP, Siris E, Bilezikian JP. A 10-year prospective study of primary hyperparathyroidism with or without parathyroid surgery. N Engl J Med. 1999;341:1249–55. - PubMed
-
- Udelsman R, Pasieka JL, Sturgeon C, Young JE, Clark OH. Surgery for asymptomatic primary hyperparathyroidism: proceedings of the third international workshop. J Clin Endocrinol Metab. 2009;94:366–72. - PubMed
-
- Zanocco K, Angelos P, Sturgeon C. Cost-effectiveness analysis of parathyroidectomy for asymptomatic primary hyperparathyroidism. Surgery. 2006;140:874–81. - PubMed
-
- Greene AB, Butler RS, McIntyre S, et al. National trends in parathyroid surgery from 1998 to 2008: a decade of change. J Am Coll Surg. 2009;209:332–43. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
