

Pediatric versus adult drug trials for conditions with high pediatric disease burden
- PMID: 22826574
- PMCID: PMC3408692
- DOI: 10.1542/peds.2012-0139
Pediatric versus adult drug trials for conditions with high pediatric disease burden
Abstract
Background and objective: Optimal treatment decisions in children require sufficient evidence on the safety and efficacy of pharmaceuticals in pediatric patients. However, there is concern that not enough trials are conducted in children and that pediatric trials differ from those performed in adults. Our objective was to measure the prevalence of pediatric studies among clinical drug trials and compare trial characteristics and quality indicators between pediatric and adult drug trials.
Methods: For conditions representing a high burden of pediatric disease, we identified all drug trials registered in ClinicalTrials.gov with start dates between 2006 and 2011 and tracked the resulting publications. We measured the proportion of pediatric trials and subjects for each condition and compared pediatric and adult trial characteristics and quality indicators.
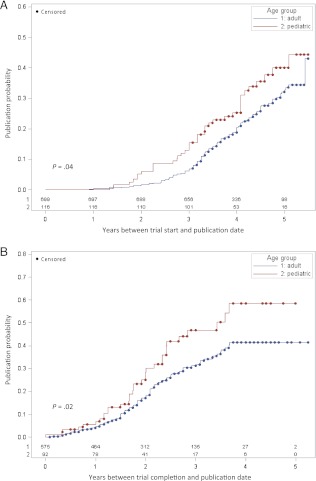
Results: For the conditions selected, 59.9% of the disease burden was attributable to children, but only 12.0% (292/2440) of trials were pediatric (P < .001). Among pediatric trials, 58.6% were conducted without industry funding compared with 35.0% of adult trials (P < .001). Fewer pediatric compared with adult randomized trials examined safety outcomes (10.1% vs 16.9%, P = .008). Pediatric randomized trials were slightly more likely to be appropriately registered before study start (46.9% vs 39.3%, P = .04) and had a modestly higher probability of publication in the examined time frame (32.8% vs 23.2%, P = .04).
Conclusions: There is substantial discrepancy between pediatric burden of disease and the amount of clinical trial research devoted to pediatric populations. This may be related in part to trial funding, with pediatric trials relying primarily on government and nonprofit organizations.
Figures
References
-
- Pandolfini C, Bonati M. A literature review on off-label drug use in children. Eur J Pediatr. 2005;164(9):552–558 - PubMed
-
- Shah SS, Hall M, Goodman DM, et al. . Off-label drug use in hospitalized children. Arch Pediatr Adolesc Med. 2007;161(3):282–290 - PubMed
-
- Caldwell PH, Murphy SB, Butow PN, Craig JC. Clinical trials in children. Lancet. 2004;364(9436):803–811 - PubMed
-
- Smyth RL, Weindling AM. Research in children: ethical and scientific aspects. Lancet. 1999;354(suppl 2):SII21–SII24 - PubMed
-
- Steinbrook R. Testing medications in children. N Engl J Med. 2002;347(18):1462–1470 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
