

Radiosurgery for high-grade glioma
- PMID: 22826815
- PMCID: PMC3400492
- DOI: 10.4103/2152-7806.95423
Radiosurgery for high-grade glioma
Abstract
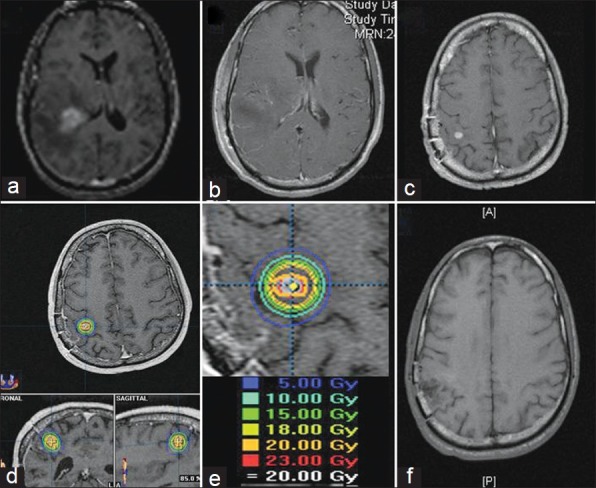
Background: For patients with newly diagnosed high-grade gliomas (HGG), the current standard-of-care treatment involves surgical resection, followed by concomitant temozolomide (TMZ) and external beam radiation therapy (XRT), and subsequent TMZ chemotherapy. For patients with recurrent HGG, there is no standard of care. Stereotactic radiosurgery (SRS) is used to deliver focused, relatively large doses of radiation to a small, precisely defined target. Treatment is usually delivered in a single fraction, but may be delivered in up to five fractions. The role of SRS in the management of patients with HGG is not well established.
Methods: The PubMed database was searched with combinations of relevant MESH headings and limits. Case reports and/or small case series were excluded. Attention was focused on overall median survival as an objective measure, and data were examined separately for newly diagnosed and recurrent HGG.
Results: With respect to newly diagnosed HGG, there is strong evidence that addition of an SRS boost prior to standard XRT provides no survival benefit. However, recent retrospective evidence suggests a possible survival benefit when SRS is performed after XRT. With respect to recurrent HGG, there is suggestion that SRS may confer a survival benefit but with potentially higher complication rates. Newer studies are investigating the combination of SRS with targeted molecular agents. Controlled prospective clinical trials using advanced imaging techniques are necessary for a complete assessment.
Conclusions: SRS has the potential to provide a survival benefit for patients with HGG. Further research is clearly warranted to define its role in the management of newly diagnosed and recurrent HGG.
Keywords: Glioma; high-grade; newly diagnosed; recurrent; stereotactic radiosurgery.
Figures
References
-
- Alexiou GA, Tsiouris S, Kyritsis AP, Voulgaris S, Argyropoulou MI, Fotopoulos AD. Glioma recurrence versus radiation necrosis: Accuracy of current imaging modalities. J Neurooncol. 2009;95:1–11. - PubMed
-
- Andrews DA, Bednarz G, Evans JJ, Downes B. A review of 3 current radiosurgery systems. Surg Neurol. 2006;66:559–64. - PubMed
-
- Anker CJ, Hymas RV, Hazard LJ, Boucher KM, Jensen RL, Shrieve DC. Stereotactic radiosurgery eligibility and selection bias in the treatment of glioblastoma multiforme. J Neurooncol. 2010;98:253–63. - PubMed
-
- Barker F, Chang S, Gutin P, Malec M, Mcdermott M, Prados M, et al. Survival and functional status after resection of recurrent glioblastoma multiforme. Neurosurgery. 1998;42:709–20. - PubMed
-
- Barnett GH, Linskey ME, Adler JR, Cozzens JW, Friedman WA, Heilburn MP, et al. Stereotactic radiosurgery-an organized neurosurgery-sanctioned definition. J Neurosurg. 2007;106:1–5. - PubMed
LinkOut - more resources
Full Text Sources
