

A physiotherapist-delivered integrated exercise and pain coping skills training intervention for individuals with knee osteoarthritis: a randomised controlled trial protocol
- PMID: 22828288
- PMCID: PMC3524463
- DOI: 10.1186/1471-2474-13-129
A physiotherapist-delivered integrated exercise and pain coping skills training intervention for individuals with knee osteoarthritis: a randomised controlled trial protocol
Abstract
Background: Knee osteoarthritis (OA) is a prevalent chronic musculoskeletal condition with no cure. Pain is the primary symptom and results from a complex interaction between structural changes, physical impairments and psychological factors. Much evidence supports the use of strengthening exercises to improve pain and physical function in this patient population. There is also a growing body of research examining the effects of psychologist-delivered pain coping skills training (PCST) particularly in other chronic pain conditions. Though typically provided separately, there are symptom, resource and personnel advantages of exercise and PCST being delivered together by a single healthcare professional. Physiotherapists are a logical choice to be trained to deliver a PCST intervention as they already have expertise in administering exercise for knee OA and are cognisant of the need for a biopsychosocial approach to management. No studies to date have examined the effects of an integrated exercise and PCST program delivered solely by physiotherapists in this population. The primary aim of this multisite randomised controlled trial is to investigate whether an integrated 12-week PCST and exercise treatment program delivered by physiotherapists is more efficacious than either program alone in treating pain and physical function in individuals with knee OA.
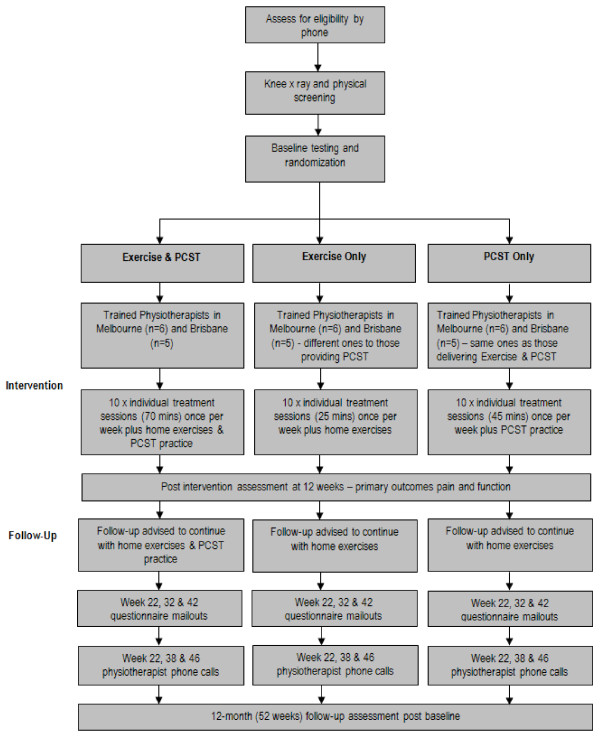
Methods/design: This will be an assessor-blinded, 3-arm randomised controlled trial of a 12-week intervention involving 10 physiotherapy visits together with home practice. Participants with symptomatic and radiographic knee OA will be recruited from the community in two cities in Australia and randomized into one of three groups: exercise alone, PCST alone, or integrated PCST and exercise. Randomisation will be stratified by city (Melbourne or Brisbane) and gender. Primary outcomes are overall average pain in the past week measured by a Visual Analogue Scale and physical function measured by the Western Ontario and McMaster Universities Osteoarthritis Index subscale. Secondary outcomes include global rating of change, muscle strength, functional performance, physical activity levels, health related quality of life and psychological factors. Measurements will be taken at baseline and immediately following the intervention (12 weeks) as well as at 32 weeks and 52 weeks to examine maintenance of any intervention effects. Specific assessment of adherence to the treatment program will also be made at weeks 22 and 42. Relative cost-effectiveness will be determined from health service usage and outcome data.
Discussion: The findings from this randomised controlled trial will provide evidence for the efficacy of an integrated PCST and exercise program delivered by physiotherapists in the management of painful and functionally limiting knee OA compared to either program alone.
Trial registration: Australian New Zealand Clinical Trials Registry reference number: ACTRN12610000533099.
References
-
- Access Economics. Painful Realities: The economic impact of arthritis in Australia. Access Economics Pty, Ltd, Canberra; 2007. pp. 1–90.
-
- Ettinger WH, Davis MA, Neuhaus JM, Mallon KP. Long-term physical functioning in persons with knee osteoarthritis from NHANES. I: Effects of comorbid medical conditions. J Clin Epidemiol. 1994;47:809–815. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
