

Global trends in antiretroviral resistance in treatment-naive individuals with HIV after rollout of antiretroviral treatment in resource-limited settings: a global collaborative study and meta-regression analysis
- PMID: 22828485
- PMCID: PMC3790969
- DOI: 10.1016/S0140-6736(12)61038-1
Global trends in antiretroviral resistance in treatment-naive individuals with HIV after rollout of antiretroviral treatment in resource-limited settings: a global collaborative study and meta-regression analysis
Erratum in
- Lancet. 2012 Oct 6;380(9849):1230
Abstract
Background: The emergence and spread of high levels of HIV-1 drug resistance in resource-limited settings where combination antiretroviral treatment has been scaled up could compromise the effectiveness of national HIV treatment programmes. We aimed to estimate changes in the prevalence of HIV-1 drug resistance in treatment-naive individuals with HIV since initiation of rollout in resource-limited settings.
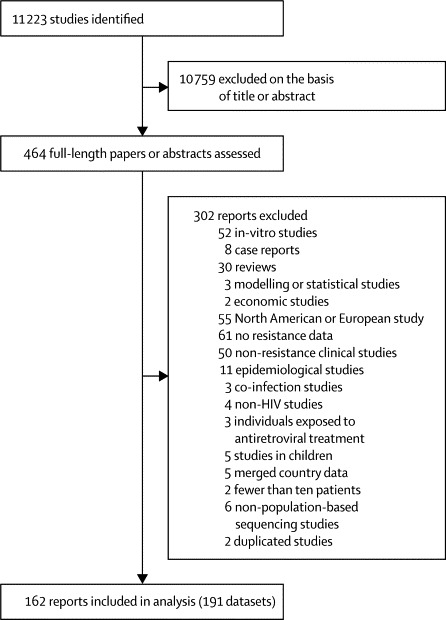
Methods: We did a systematic search for studies and conference abstracts published between January, 2001, and July, 2011, and included additional data from the WHO HIV drug resistance surveillance programme. We assessed the prevalence of drug-resistance mutations in untreated individuals with respect to time since rollout in a series of random-effects meta-regression models.
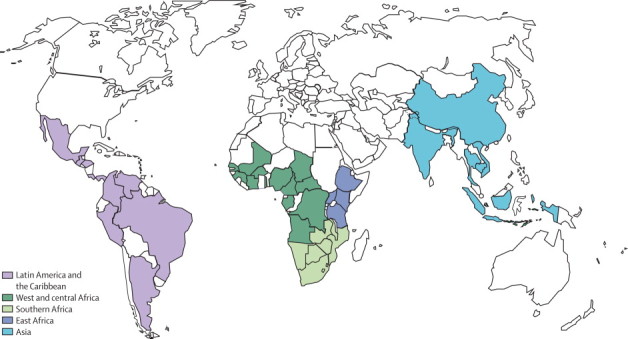
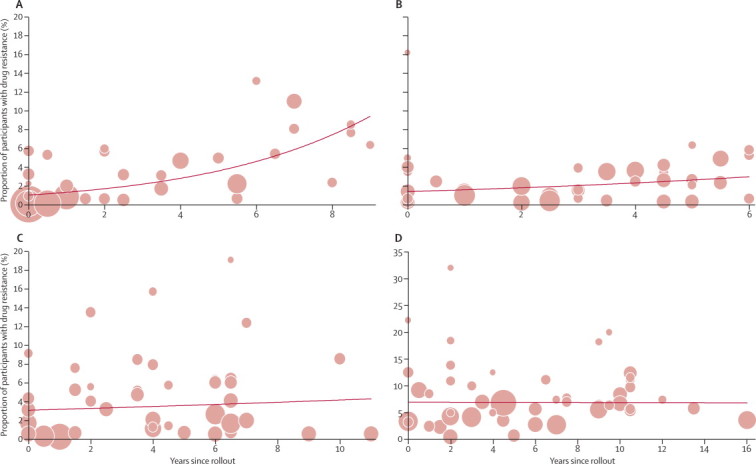
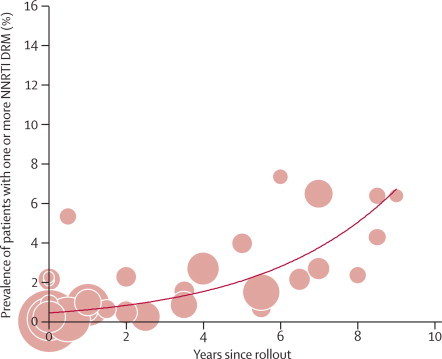
Findings: Study-level data were available for 26,102 patients from sub-Saharan Africa, Asia, and Latin America. We recorded no difference between chronic and recent infection on the prevalence of one or more drug-resistance mutations for any region. East Africa had the highest estimated rate of increase at 29% per year (95% CI 15 to 45; p=0·0001) since rollout, with an estimated prevalence of HIV-1 drug resistance at 8 years after rollout of 7·4% (4·3 to 12·7). We recorded an annual increase of 14% (0% to 29%; p=0·054) in southern Africa and a non-significant increase of 3% (-0·9 to 16; p=0·618) in west and central Africa. There was no change in resistance over time in Latin America, and because of much country-level heterogeneity the meta-regression analysis was not appropriate for Asia. With respect to class of antiretroviral, there were substantial increases in resistance to non-nucleoside reverse transcriptase inhibitors (NNRTI) in east Africa (36% per year [21 to 52]; p<0·0001) and southern Africa (23% per year [7 to 42]; p=0·0049). No increase was noted for the other drug classes in any region.
Interpretation: Our findings suggest a significant increase in prevalence of drug resistance over time since antiretroviral rollout in regions of sub-Saharan Africa; this rise is driven by NNRTI resistance in studies from east and southern Africa. The findings are of concern and draw attention to the need for enhanced surveillance and drug-resistance prevention efforts by national HIV treatment programmes. Nevertheless, estimated levels, although increasing, are not unexpected in view of the large expansion of antiretroviral treatment coverage seen in low-income and middle-income countries--no changes in antiretroviral treatment guidelines are warranted at the moment.
Funding: Bill & Melinda Gates Foundation and the European Community's Seventh Framework Programme.
Copyright © 2012 Elsevier Ltd. All rights reserved.
Figures
Comment in
-
Antiretroviral drug resistance in resource-limited settings.Lancet. 2012 Oct 6;380(9849):1210-1. doi: 10.1016/S0140-6736(12)61188-X. Epub 2012 Jul 23. Lancet. 2012. PMID: 22828483 No abstract available.
References
-
- Gilks CF, Crowley S, Ekpini R. The WHO public-health approach to antiretroviral treatment against HIV in resource-limited settings. Lancet. 2006;368:505–510. - PubMed
-
- WHO Antiretroviral therapy for HIV infection in adults and adolescents—recommendations for a public health approach: 2010 revision. http://www.who.int/hiv/pub/arv/adult2010/en/index.html (accessed July 1, 2011). - PubMed
-
- Together we will end AIDS. Joint United Nations Programme on HIV/AIDS. 2012. http://www.unaids.org/en/media/unaids/contentassets/documents/epidemiolo... (accessed July 18, 2012).
-
- Barth RE, van der Loeff MF, Schuurman R, Hoepelman AI, Wensing AM. Virological follow-up of adult patients in antiretroviral treatment programmes in sub-Saharan Africa: a systematic review. Lancet Infect Dis. 2010;10:155–166. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
