

Ki-67 labeling index as an adjunct in the diagnosis of serous tubal intraepithelial carcinoma
- PMID: 22833080
- PMCID: PMC3715095
- DOI: 10.1097/PGP.0b013e31824cbeb4
Ki-67 labeling index as an adjunct in the diagnosis of serous tubal intraepithelial carcinoma
Abstract
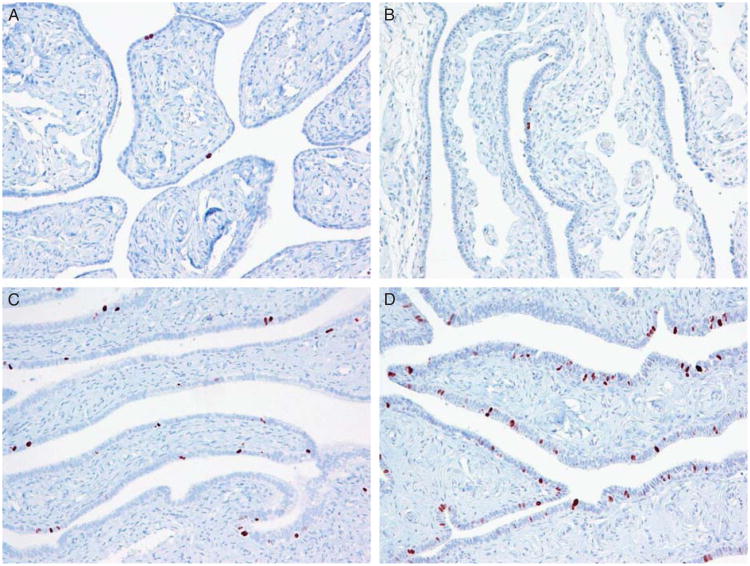
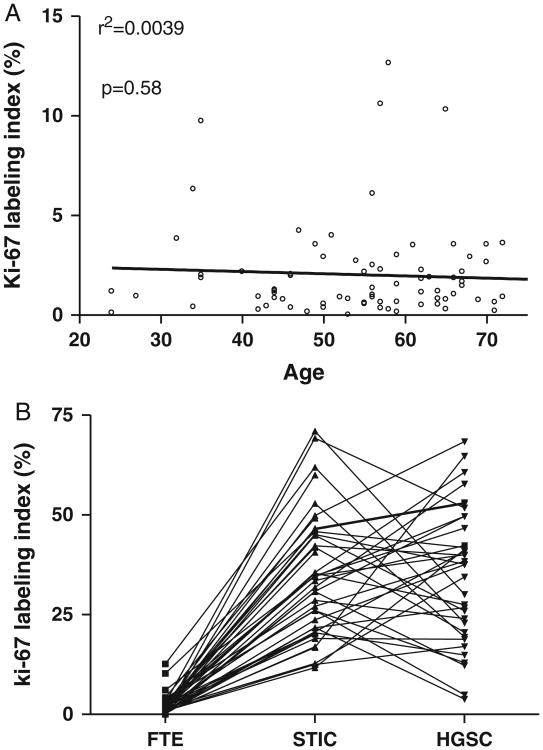
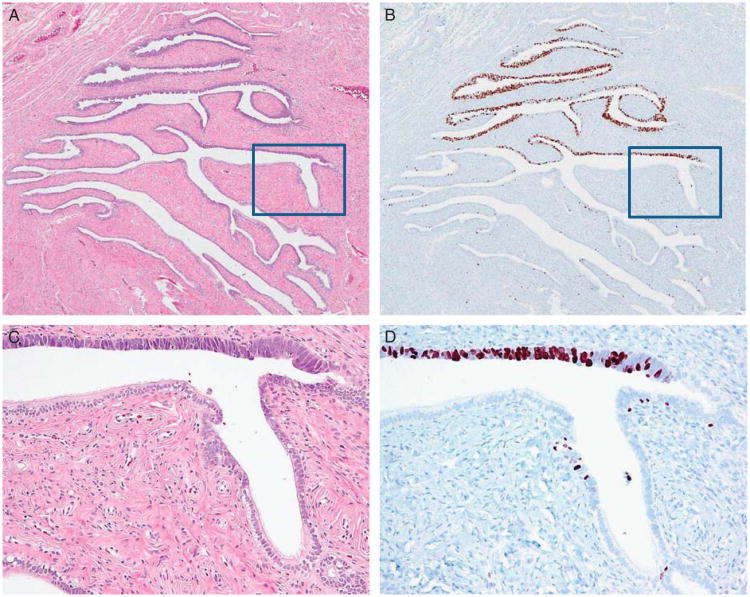
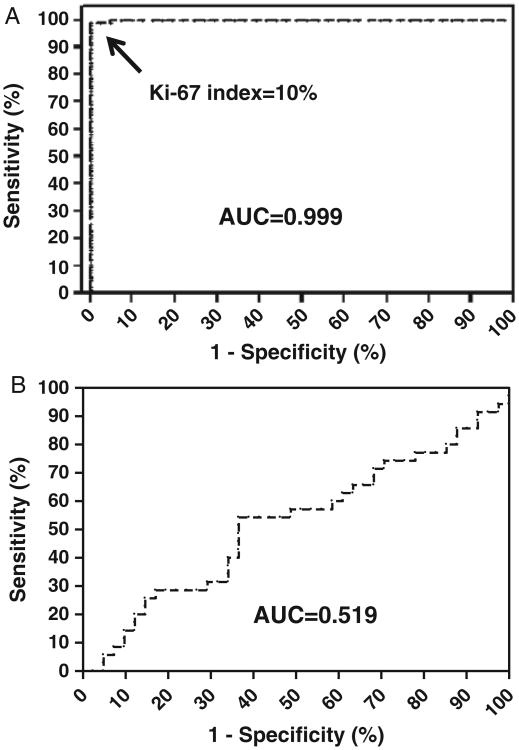
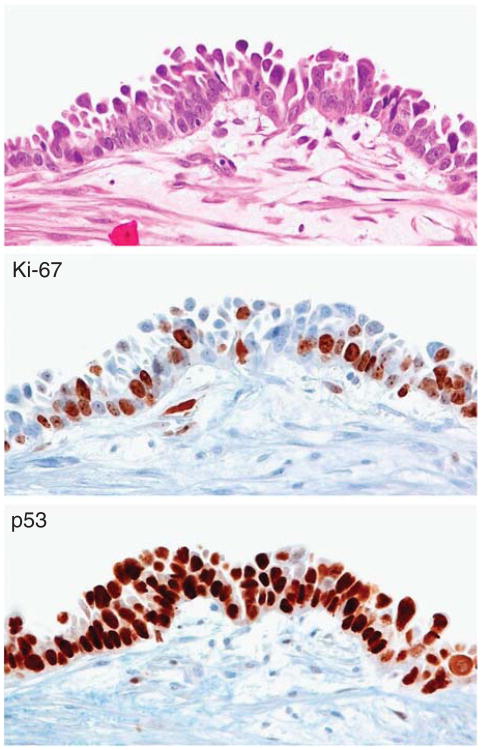
There is mounting evidence that serous tubal intraepithelial carcinoma (STIC) may be the immediate precursor of ovarian high-grade serous carcinoma (HGSC) but the criteria for its diagnosis are not well established as highlighted in a recent study showing that interobserver reproducibility, even among expert gynecologic pathologists, was moderate at best. Given the clinical significance of a diagnosis of STIC in a patient who has no other evidence of ovarian carcinoma, this is a serious issue that we felt needed to be addressed. Although it is not clear, at this time, whether such a patient should or should not be treated, the importance of an accurate and reproducible diagnosis of precursors of ovarian carcinoma cannot be underestimated. We hypothesized that an elevated Ki-67 labeling index may aid the diagnosis of STIC. Accordingly, we compared the Ki-67 index of STIC and HGSC to normal fallopian tube epithelium (FTE) in the same patients and to a control group of patients without carcinoma, matched for age. A total of 41 STICs were analyzed, of which 35 were associated with a concurrent HGSC. In FTE, immunoreactivity for Ki-67 was restricted to a few scattered cells (mean 2.0%). No statistically significant difference was found between patients with and without HGSC (P>0.05). However, both STICs and HGSC had significantly higher Ki-67 indices than normal FTE (P<0.0001). STICs uniformly had an elevated Ki-67 labeling index that ranged from 11.7% to 71.1% (average 35.6%). There was no correlation of the Ki-67 labeling index in the STICs and the associated HGSC, as the labeling index was lower in STIC in 18/35 (51.4%) whereas it was higher in 17/35 (48.6%) (P=0.86). In conclusion, the findings in this study indicate that compared with FTE, STICs have a significantly higher Ki-67 index similar to HGSC. Accordingly, the Ki-67 index can aid the diagnosis of intraepithelial tubal proliferations suspicious for STIC. Therefore, we propose that a Ki-67 index of 10% is a useful diagnostic tool to distinguish STICs from normal FTE.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Kindelberger DW, Lee Y, Miron A, et al. Intraepithelial carcinoma of the fimbria and pelvic serous carcinoma: Evidence for a causal relationship. Am J Surg Pathol. 2007;31:161–9. - PubMed
-
- Carlson JW, Jarboe EA, Kindelberger D, et al. Serous tubal intraepithelial carcinoma: diagnostic reproducibility and its implications. Int J Gynecol Pathol. 2010;29:310–4. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
