

Case Reports
doi: 10.1093/icvts/ivs325.
Epub 2012 Jul 25.
Ultrasound-guided thoracotomy for implantation of an epicardial left ventricular lead after left pneumonectomy
Affiliations
- PMID: 22833507
- PMCID: PMC3480600
- DOI: 10.1093/icvts/ivs325
Item in Clipboard
Case Reports
Ultrasound-guided thoracotomy for implantation of an epicardial left ventricular lead after left pneumonectomy
Interact Cardiovasc Thorac Surg.
2012 Nov.
Abstract
Surgical placement of a left ventricular epicardial pacing lead is a valuable alternative to the standard approach of endovascular placement of a pacing lead in the coronary sinus for cardiac resynchronization therapy. Despite higher perioperative morbidity, surgically placed leads perform well with lower revision and dislocation rates. Moreover, surgery is the only option when an endovascular approach proves to be unsuccessful. We report a successful implantation of an epicardial left ventricular lead through an ultrasound-guided lateral left mini-thoracotomy in a patient with a severely disturbed thoracic anatomy due to left pneumonectomy.
Figures
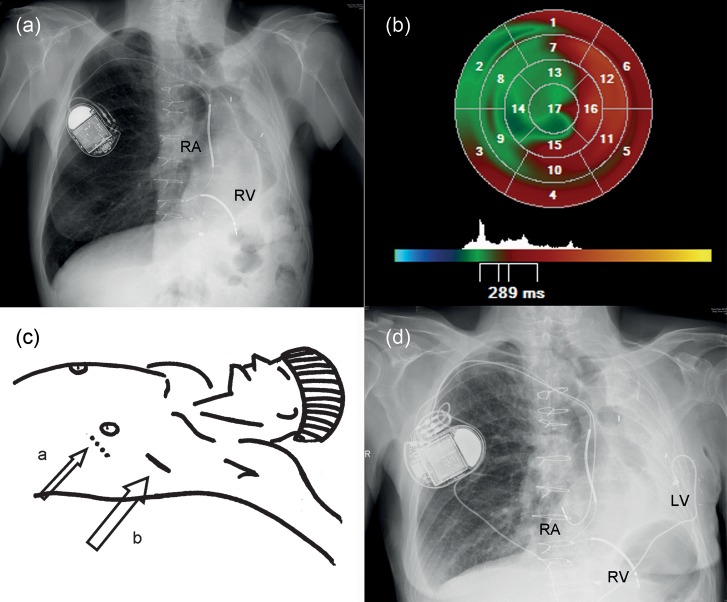
(a) Chest X-ray showing an extreme leftward displacement of the heart, right atrial (RA) and right ventricular (RV)—shock lead connected to the internal cardiac defibrillator-CRT in the right infraclavicular region. (b) LV dyssynchrony analysis from an RT3DE data set using parametric images. The global time to minimum systolic volume is used as timing reference; early segments are coded in blue, whereas late segments are coded in red. (c) a: conventional site for incision and; b: actual skin incision based on ultrasound guidance. (d) Postoperative chest X-ray with the LV-lead tunnelled around the xyphoid processus.
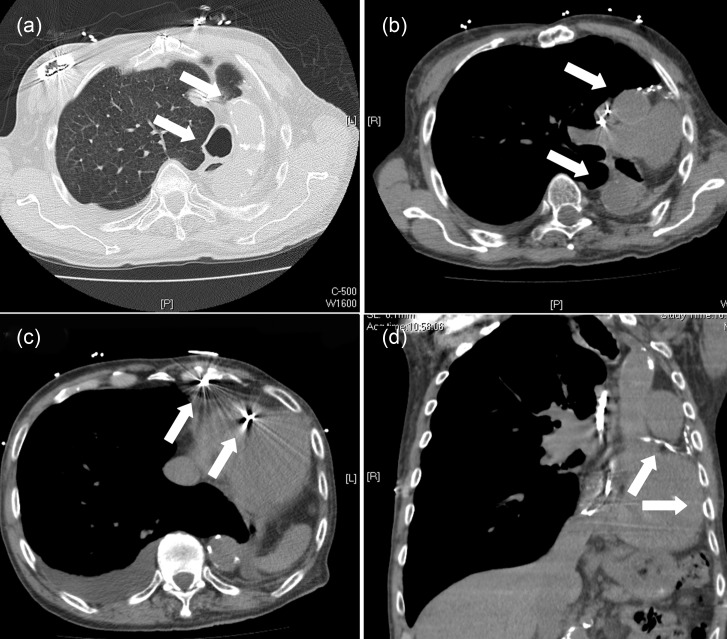
(a) CT scan: enlargement of the right lung, lateral displacement of trachea and calcified aorta. (b) CT scan: lateral displaced of the heart and great vessels. (c) CT scan: pacemaker leads in the right atrium and shock-lead in the right ventricle. (d) CT scan: calcified venous bypass, left ventricle adjacent to the thoracic wall.
Similar articles
-
Electrically vs. imaging-guided left ventricular lead placement in cardiac resynchronization therapy: a randomized controlled trial.Europace. 2019 Sep 1;21(9):1369-1377. doi: 10.1093/europace/euz184. Europace. 2019. PMID: 31274152 Clinical Trial.
-
Reverse ventricular remodeling and long-term survival in patients undergoing cardiac resynchronization with surgically versus percutaneously placed left ventricular pacing leads.Heart Rhythm. 2015 Mar;12(3):517-523. doi: 10.1016/j.hrthm.2014.11.013. Epub 2014 Nov 13. Heart Rhythm. 2015. PMID: 25460866
-
A hybrid approach to cardiac resynchronization therapy.Ann Thorac Cardiovasc Surg. 2011;17(3):273-6. doi: 10.5761/atcs.oa.10.01597. Ann Thorac Cardiovasc Surg. 2011. PMID: 21697789
-
Clinical outcome of left ventricular multipoint pacing versus conventional biventricular pacing in cardiac resynchronization therapy: a systematic review and meta-analysis.Heart Fail Rev. 2018 Nov;23(6):927-934. doi: 10.1007/s10741-018-9737-5. Heart Fail Rev. 2018. PMID: 30209643
-
Optimizing cardiac resynchronization therapy for congestive heart failure.Curr Probl Cardiol. 2013 Jun;38(6):215-37. doi: 10.1016/j.cpcardiol.2013.03.003. Curr Probl Cardiol. 2013. PMID: 23664171 Review.
Cited by
-
In vitro and in vivo studies on the biocompatibility of a self-powered pacemaker with a flexible buckling piezoelectric vibration energy harvester for rats.Ann Transl Med. 2021 May;9(9):800. doi: 10.21037/atm-21-1707. Ann Transl Med. 2021. PMID: 34268413 Free PMC article.
References
-
- Marsan NA, Bleeker GB, Ypenburg C, Ghio S, van de Veire NR, Holman ER, et al. Real-time three-dimensional echocardiography permits quantification of left ventricular mechanical dyssynchrony and predicts acute response to cardiac resynchronization therapy. J Cardiovasc Electrophysiol. 2008;19:392–9. - PubMed
-
- Coceani M. Guideline challenge: has CRT earned a Class I recommendation? Circ Heart Fail. 2010;3:460–1. - PubMed
-
- Navia JL, Atik FA, Grimm RA, Garcia M, Vega PR, Myhre U, et al. Minimally invasive left ventricular epicardial lead placement: surgical techniques for heart failure resynchronization therapy. Ann Thorac Surg. 2005;79:1536–44. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
