

Screening for colorectal cancer and advanced colorectal neoplasia in kidney transplant recipients: cross sectional prevalence and diagnostic accuracy study of faecal immunochemical testing for haemoglobin and colonoscopy
- PMID: 22833618
- PMCID: PMC3404596
- DOI: 10.1136/bmj.e4657
Screening for colorectal cancer and advanced colorectal neoplasia in kidney transplant recipients: cross sectional prevalence and diagnostic accuracy study of faecal immunochemical testing for haemoglobin and colonoscopy
Abstract
Objective: To investigate whether screening kidney transplant recipients aged over 50 years for colorectal cancer with a faecal immunochemical test for haemoglobin might be justified, by determining the prevalence of advanced colorectal neoplasia and evaluating the diagnostic accuracy of faecal haemoglobin testing compared with colonoscopy in a population of kidney transplant recipients at otherwise average risk.
Design: Cross sectional prevalence and diagnostic accuracy study with index test of faecal haemoglobin and reference standard of colonoscopy.
Setting: Outpatient clinics in metropolitan and regional hospitals in South Australia.
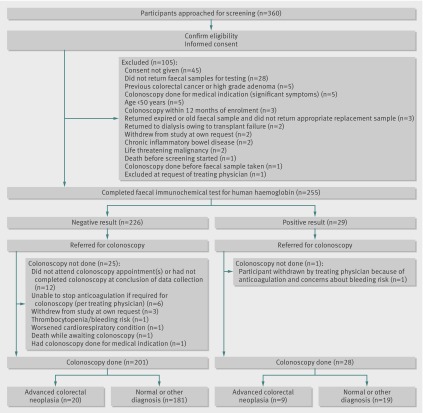
Participants: 229 kidney transplant recipients aged 50 years and over, who were at least 6 months (mean 9.0 (SD 8.4) years) post-transplant and otherwise at average risk of colorectal cancer, completed the study between June 2008 and October 2011.
Interventions: Faecal immunochemical testing (Enterix Insure) for human haemoglobin, followed by colonoscopy with histological evaluation of retrieved samples.
Main outcome measures: Prevalence of advanced colorectal neoplasia, defined as an adenoma at least 10 mm in diameter, villous features, high grade dysplasia, or colorectal cancer; sensitivity, specificity, and predictive values of faecal haemoglobin testing for advanced neoplasia compared with colonoscopy.
Results: Advanced colorectal neoplasia was found in 29 (13%, 95% confidence interval 9% to 18%) participants, including 2% (n=4) with high grade dysplasia and 2% (n=5) with colorectal cancer. Faecal testing for haemoglobin was positive in 12% (n=28); sensitivity, specificity, and positive and negative predictive values for advanced neoplasia were 31.0% (15.3% to 50.8%), 90.5% (85.6% to 94.2%), 32.1% (15.9% to 52.4%), and 90.1% (85.1% to 93.8%). Colonoscopy was well tolerated, with no significant adverse outcomes. To identify one case of advanced neoplasia, 8 (6 to 12) colonoscopies were needed.
Conclusions: Kidney transplant recipients aged over 50 years have a high prevalence of advanced colorectal neoplasia. Faecal haemoglobin screening for colorectal neoplasia has similar performance characteristics in transplant recipients to those reported in general population studies, with poor sensitivity but reasonable specificity. Surveillance colonoscopy might be a more appropriate approach in this population.
Trial registration: Australian New Zealand Clinical Trials Registry ACTRN12608000154303.
Conflict of interest statement
Competing interests: All authors have completed the Unified Competing Interest form at
Comment in
-
Detection of bowel cancer in kidney transplant recipients.BMJ. 2012 Jul 25;345:e5081. doi: 10.1136/bmj.e5081. BMJ. 2012. PMID: 22833633 No abstract available.
References
-
- McDonald SP, Russ GR. Survival of recipients of cadaveric kidney transplants compared with those receiving dialysis treatment in Australia and New Zealand, 1991-2001. Nephrol Dial Transplant 2002;17:2212-9. - PubMed
-
- McDonald SP, Excell L, Livingstone B. ANZDATA registry report. Australia and New Zealand Dialysis and Transplant Registry, 2009.
-
- Vajdic CM, McDonald SP, McCredie MR, van Leeuwen MT, Stewart JH, Law M, et al. Cancer incidence before and after kidney transplantation. JAMA 2006;296:2823-31. - PubMed
-
- Kasiske BL, Snyder JJ, Gilbertson DT, Wang C. Cancer after kidney transplantation in the United States. Am J Transplant 2004;4:905-13. - PubMed
-
- Webster AC, Craig JC, Simpson JM, Jones MP, Chapman JR. Identifying high risk groups and quantifying absolute risk of cancer after kidney transplantation: a cohort study of 15,183 recipients. Am J Transplant 2007;7:2140-51. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical