

The role of bronchodilator treatment in the prevention of exacerbations of COPD
- PMID: 22835613
- PMCID: PMC3511775
- DOI: 10.1183/09031936.00048912
The role of bronchodilator treatment in the prevention of exacerbations of COPD
Abstract
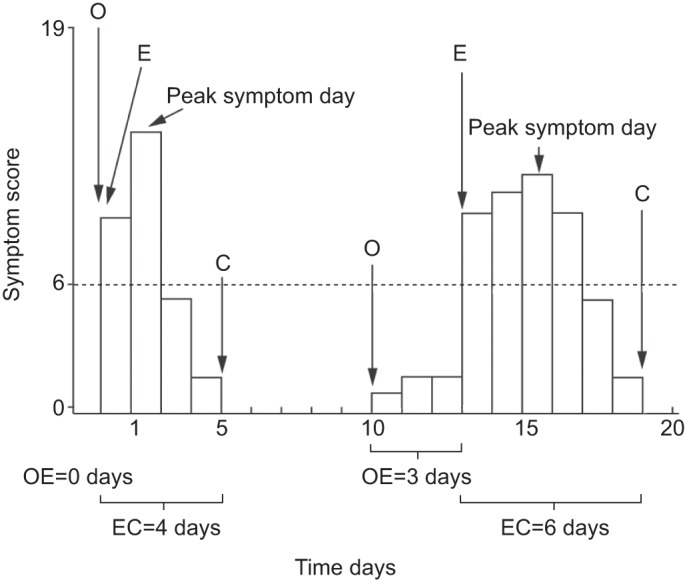
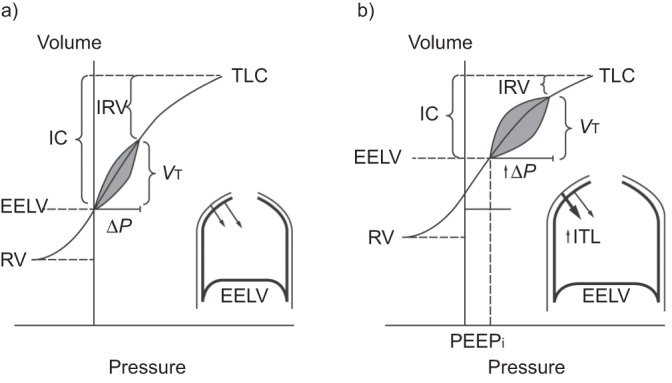
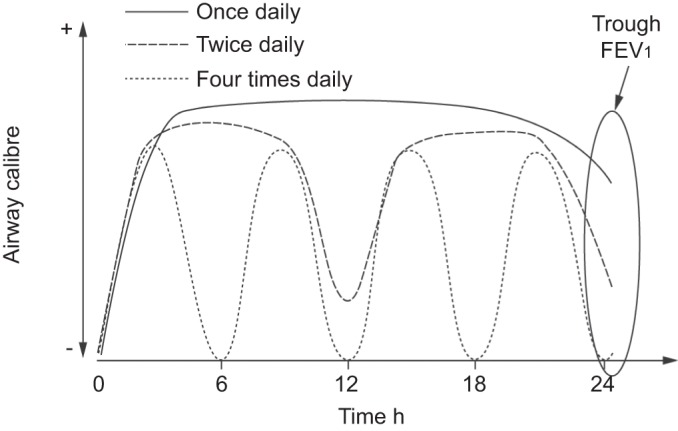
Exacerbations of chronic obstructive pulmonary disease (COPD) are natural events in the progression of the disease, and are characterised by acute worsening of symptoms, especially dyspnoea. These heterogeneous events follow increased airway inflammation, often due to infection, and lead to decreased airflow and increased lung hyperinflation relative to stable COPD. Although exacerbation frequency generally increases as COPD progresses, some patients experience frequent exacerbations (≥ 2 per year) independently of disease severity. Exacerbations, especially frequent exacerbations, are associated with impaired health-related quality of life, reduced physical activity and poor disease prognosis. The cornerstone of pharmacotherapy for stable COPD is long-acting bronchodilators, including the long-acting β(2)-agonists (LABAs) and long-acting anti-muscarinic agents (LAMAs) alone or combined with inhaled corticosteroids (ICS). While ICS treatment can potentially reduce the risk of exacerbations, clinical studies have demonstrated the efficacy of LABAs and LAMAs in reducing COPD symptoms, primarily by reducing lung hyperinflation secondary to reduced airway resistance. Sustained reduction in lung hyperinflation may in turn lessen dyspnoea during an exacerbation. Indeed, recent studies suggest that bronchodilators may also reduce the incidence of, or prevent, exacerbations. Using data from recent studies, this review explores the evidence and possible mechanisms through which bronchodilators may prevent exacerbations.
Conflict of interest statement
Statements of interest for all authors and the study itself can be found at
Figures

References
-
- World Health Organization Chronic respiratory diseases. Burden of chronic respiratory diseases. www.who.int/respiratory/copd/burden/en/index.html Date last accessed: March 19, 2012
-
- Global Initiative for Chronic Obstructive Lung Disease Global Strategy for the Diagnosis, Management and Prevention of chronic obstructive pulmonary disease. Revised 2011. www.goldcopd.org Date last updated: December 2011. Date last accessed: March 19, 2012 - PubMed
-
- O'Donnell DE, Laveneziana P. The clinical importance of dynamic lung hyperinflation in COPD. COPD 2006; 3: 219–232 - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical