

Obesity and asthma: an inflammatory disease of adipose tissue not the airway
- PMID: 22837379
- PMCID: PMC3480522
- DOI: 10.1164/rccm.201203-0573OC
Obesity and asthma: an inflammatory disease of adipose tissue not the airway
Abstract
Rationale: Obesity is a major risk factor for asthma; the reasons for this are poorly understood, although it is thought that inflammatory changes in adipose tissue in obesity could contribute to airway inflammation and airway reactivity in individuals who are obese.
Objectives: To determine if inflammation in adipose tissue in obesity is related to late-onset asthma, and associated with increased markers of airway inflammation and reactivity.
Methods: We recruited a cohort of obese women with asthma and obese control women. We followed subjects with asthma for 12 months after bariatric surgery. We compared markers in adipose tissue and the airway from subjects with asthma and control subjects, and changes in subjects with asthma over time.
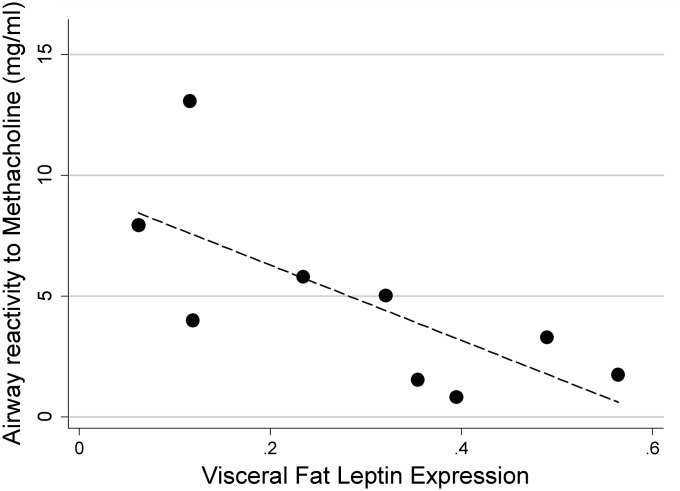
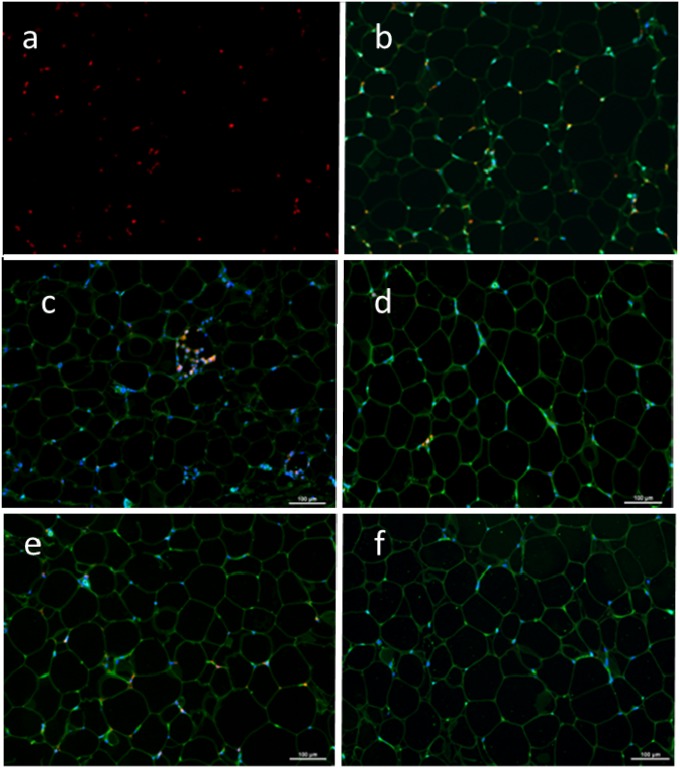
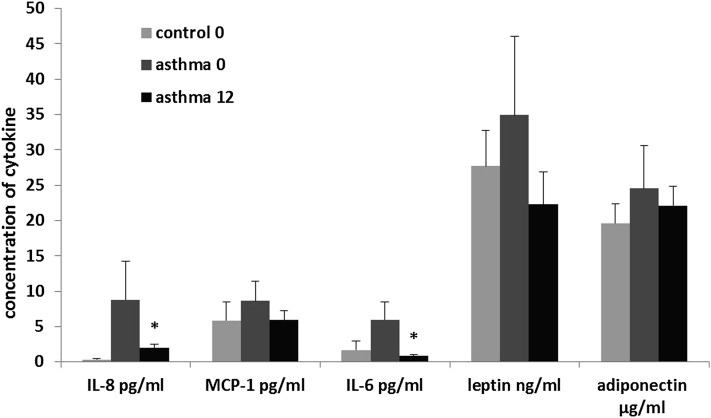
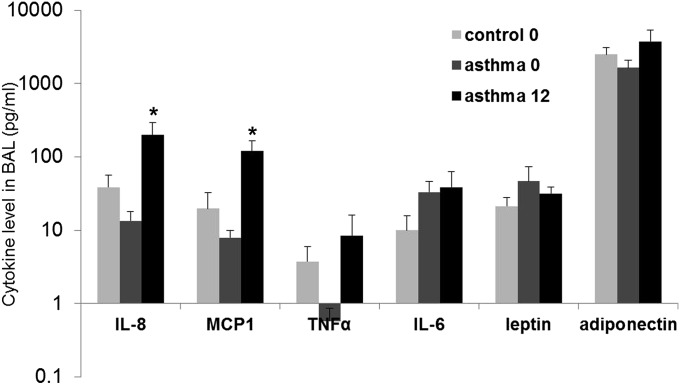
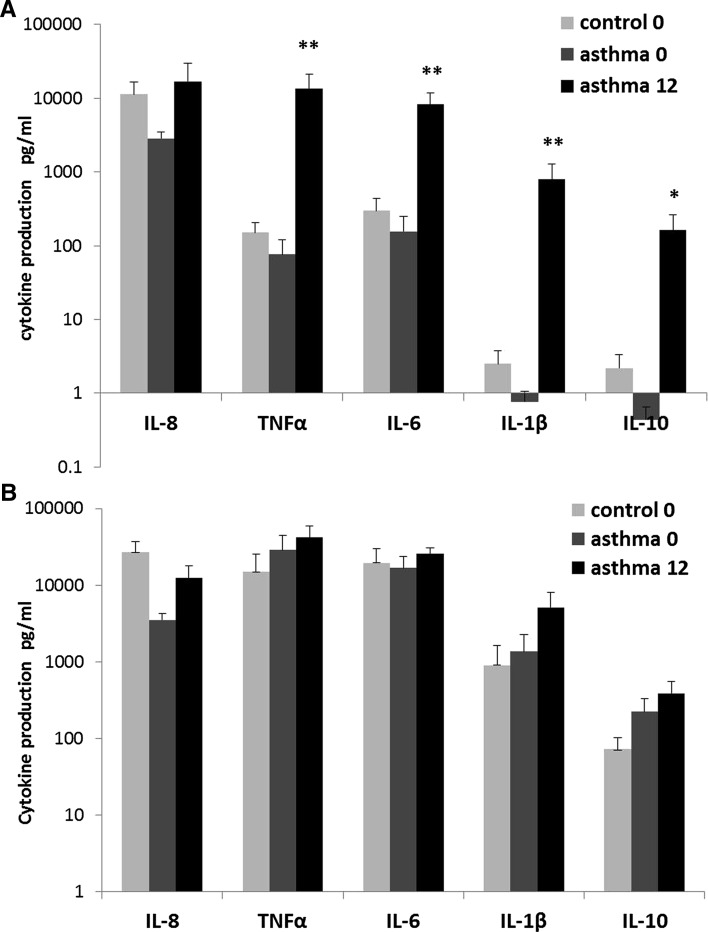
Measurements and main results: Subjects with asthma had increased macrophage infiltration of visceral adipose tissue (P < 0.01), with increased expression of leptin (P < 0.01) and decreased adiponectin (p < 0.001) when controlled for body mass index. Similar trends were observed in subcutaneous adipose tissue. Airway epithelial cells expressed receptors for leptin and adiponectin, and airway reactivity was significantly related to visceral fat leptin expression (rho = -0.8; P < 0.01). Bronchoalveolar lavage cytokines and cytokine production from alveolar macrophages were similar in subjects with asthma and control subjects at baseline, and tended to increase 12 months after surgery.
Conclusions: Obesity is associated with increased markers of inflammation in serum and adipose tissue, and yet decreased airway inflammation in obese people with asthma; these patterns reverse with bariatric surgery. Leptin and other adipokines may be important mediators of airway disease in obesity through direct effects on the airway rather than by enhancing airway inflammation.
Figures
References
-
- Camargo CA, Jr, Weiss ST, Zhang S, Willett WC, Speizer FE. Prospective study of body mass index, weight change, and risk of adult-onset asthma in women. Arch Intern Med 1999;159:2582–2588 - PubMed
-
- Mosen DM, Schatz M, Magid DJ, Camargo CA., Jr The relationship between obesity and asthma severity and control in adults. J Allergy Clin Immunol 2008;122:507–511 - PubMed
-
- Vortmann M, Eisner MD. BMI and health status among adults with asthma. Obesity (Silver Spring) 2008;16:146–152 - PubMed
-
- Taylor B, Mannino D, Brown C, Crocker D, Twum-Baah N, Holguin F. Body mass index and asthma severity in the national asthma survey. Thorax 2008;63:14–20 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
