

Transhepatic metallic stenting for hepaticojejunostomy stricture following laparoscopic cholecystectomy biliary injury: A case of successful 20 years follow-up
- PMID: 22837599
- PMCID: PMC3401726
- DOI: 10.4103/0972-9941.97599
Transhepatic metallic stenting for hepaticojejunostomy stricture following laparoscopic cholecystectomy biliary injury: A case of successful 20 years follow-up
Abstract
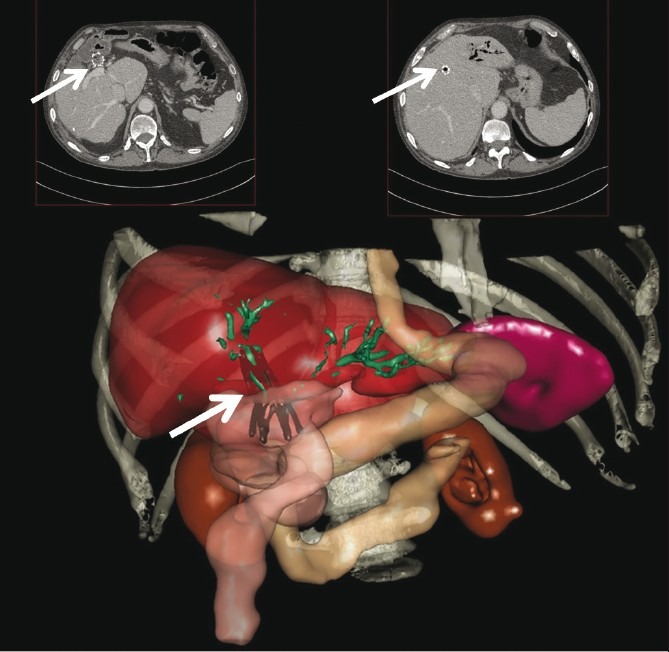
Laparoscopic cholecystectomy is still associated with a considerable rate of biliary injuries and related strictures. Advances in interventional endoscopy and percutaneous techniques have made stenting a preferred treatment modality for the management of these strictures. We report successful 20 years of follow-up of a case of trans-hepatic metallic stenting (2 Gianturco(®) prostheses, 5 cm long, 2 cm in diameter) done for stenosed hepatico-jejunostomy anastomosis after laparoscopic CBD injury. Percutaneous transhepatic stenting and long-term placement of metallic stents need to be re-evaluated as a minimally invasive definitive treatment option for benign biliary strictures in patients with altered anatomy such as hepatico-jejunostomy or in whom re-operation involves high risk.
Keywords: Biliary SEMS; hepatico-jejunostomy stricture; iatrogenic bile duct injuries; metallic biliary stents; percutaneous transhepatic biliary stenting; postoperative biliary strictures.
Conflict of interest statement
Figures

References
-
- Vecchio R, MacFadyen BV, Latteri S. Laparoscopic cholecystectomy: An analysis on 114,005 cases of United States series. Int Surg. 1998;83:215–9. - PubMed
-
- Costamagna G, Shah SK, Tringali A. Current management of postoperative complications and benign biliary strictures. Gastrointest Endosc Clin N Am. 2003;13:635–48. 9. - PubMed
-
- Isayama H, Nakai Y, Togawa O, Kogure H, Ito Y, Sasaki T, et al. Covered metallic stents in the management of malignant and benign pancreatobiliary strictures. J Hepatobiliary Pancreat Surg. 2009;16:624–7. - PubMed
-
- Misra S, Melton GB, Geschwind JF, Venbrux AC, Cameron JL, Lillemoe KD. Percutaneous management of bile duct strictures and injuries associated with laparoscopic cholecystectomy: A decade of experience. J Am Coll Surg. 2004;198:218–26. - PubMed
Publication types
LinkOut - more resources
Full Text Sources