

Mast cell number, phenotype, and function in human pulmonary arterial hypertension
- PMID: 22837863
- PMCID: PMC3401876
- DOI: 10.4103/2045-8932.97609
Mast cell number, phenotype, and function in human pulmonary arterial hypertension
Abstract
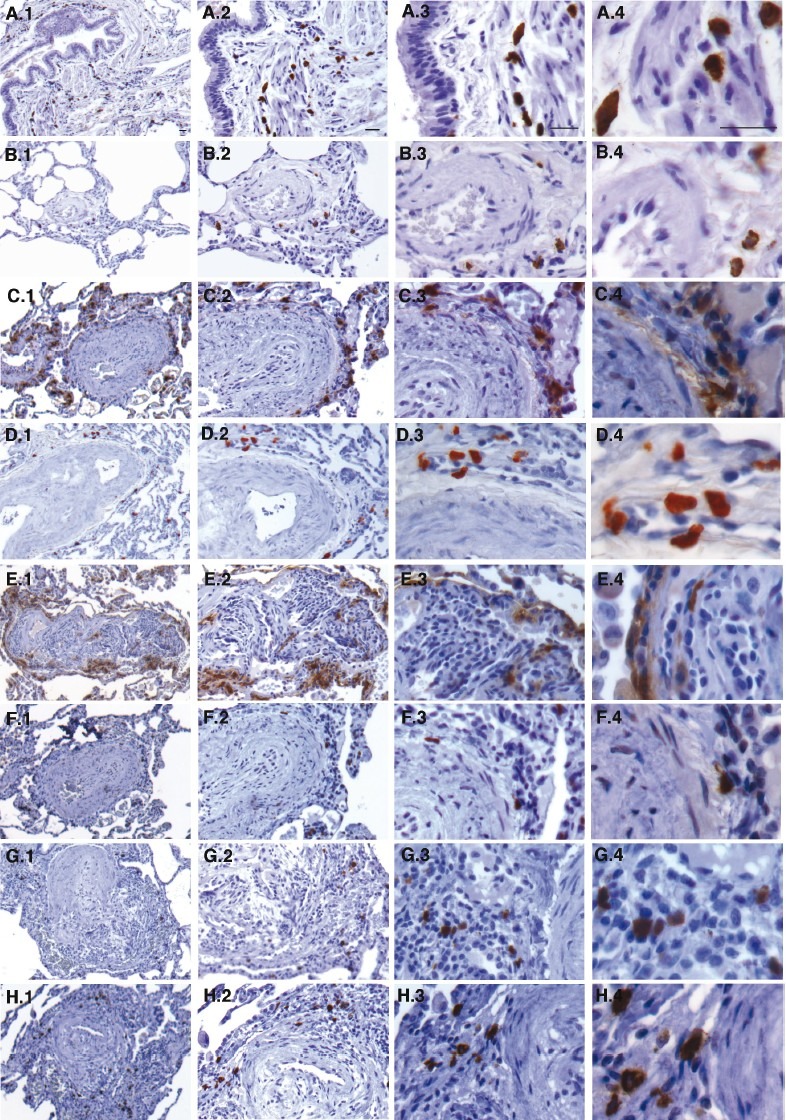
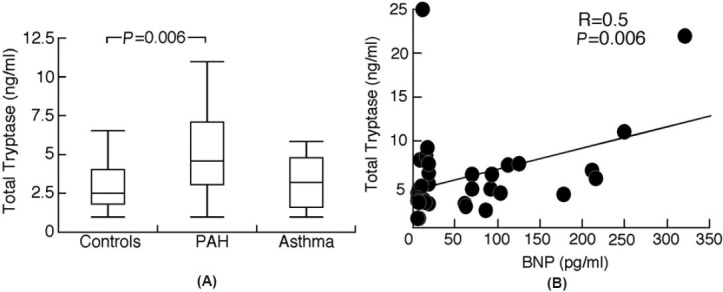
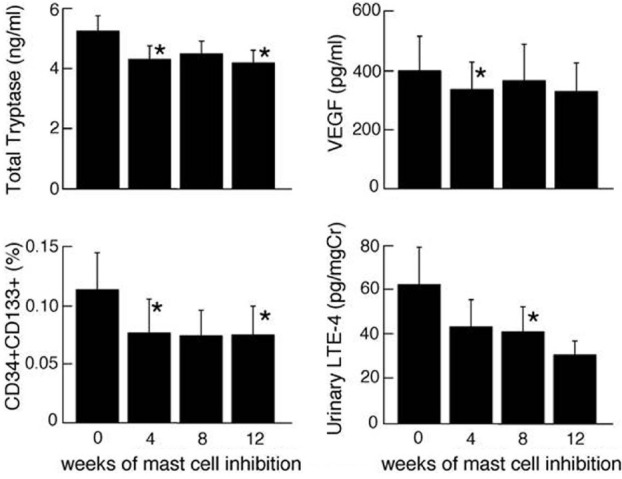
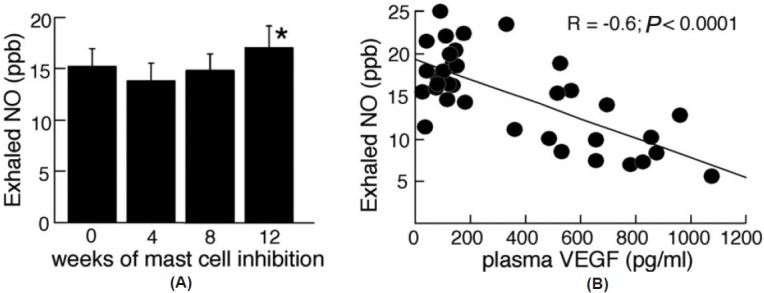
A proliferation of mast cells around the small pulmonary blood vessels and the alveolar septae has been noted in models of pulmonary hypertension, and in plexiform lesions of pulmonary arterial hypertension (PAH) in patients. Here, we hypothesize that total mast cell numbers and activation are increased in PAH and that they contribute to vascular remodeling through cellular and soluble proangiogenic effectors. To test this, blood and urine were collected from patients with PAH (N=44), asthma (N=18) and healthy controls (N=29) to quantitate biomarkers of total body mast cell numbers and activation (total and mature tryptase, N-methyl histamine, leukotriene LTE(4) and prostaglandin PGD-M). Serum total tryptase was higher in PAH than that in controls suggesting greater numbers of mast cells, but indicators of mast cell activation (mature tryptase, LTE(4) and PGD-M) were similar among PAH, asthma, and controls. Immunohistochemistry of lung tissues identified mast cells as primarily perivascular and connective tissue chymase(+) type in PAH, rather than mucosal phenotype. Intervention with mast cell inhibitors cromolyn and fexofenadine was performed in 9 patients for 12 weeks to identify the influence of mast cell products on the pathologic proangiogenic environment. Treatment decreased total tryptase and LTE-4 levels over time of treatment. This occurred in parallel to a drop in vascular endothelial growth factor (VEGF) and circulating proangiogenic CD34+CD133+ progenitor cells, which suggests that mast cells may promote vascular remodeling and dysfunction. In support of this, levels of exhaled nitric oxide, a vasodilator that is generally low in PAH, increased at the end of the 12-week mast cell blockade and antihistamine. These results suggest that mast cells might contribute to the pulmonary vascular pathologic processes underlying PAH. More studies are needed to confirm their potential contribution to the disease.
Keywords: mast cells; proangiogenic progenitor cells; pulmonary arterial hypertension; tryptase.
Conflict of interest statement
Figures
References
-
- Farber HW, Loscalzo J. Pulmonary arterial hypertension. The New England journal of medicine. 2004;351:1655–65. - PubMed
-
- Humbert M, McLaughlin VV. The 4th World Symposium on Pulmonary Hypertension.Introduction. J Am Coll Cardiol. 2009;54(1 Suppl):S1–2. - PubMed
-
- McLaughlin VV, McGoon MD. Pulmonary arterial hypertension. Circulation. 2006;114:1417–31. - PubMed
-
- Humbert M, Sitbon O, Chaouat A, Bertocchi M, Habib G, Gressin V, et al. Survival in patients with idiopathic, familial, and anorexigen-associated pulmonary arterial hypertension in the modern management era. Circulation. 2010;122:156–63. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
