

Left ventricular remodeling and hypertrophy in patients with aortic stenosis: insights from cardiovascular magnetic resonance
- PMID: 22839417
- PMCID: PMC3457907
- DOI: 10.1186/1532-429X-14-50
Left ventricular remodeling and hypertrophy in patients with aortic stenosis: insights from cardiovascular magnetic resonance
Abstract
Background: Cardiovascular magnetic resonance (CMR) is the gold standard non-invasive method for determining left ventricular (LV) mass and volume but has not been used previously to characterise the LV remodeling response in aortic stenosis. We sought to investigate the degree and patterns of hypertrophy in aortic stenosis using CMR.
Methods: Patients with moderate or severe aortic stenosis, normal coronary arteries and no other significant valve lesions or cardiomyopathy were scanned by CMR with valve severity assessed by planimetry and velocity mapping. The extent and patterns of hypertrophy were investigated using measurements of the LV mass index, indexed LV volumes and the LV mass/volume ratio. Asymmetric forms of remodeling and hypertrophy were defined by a regional wall thickening ≥ 13 mm and >1.5-fold the thickness of the opposing myocardial segment.
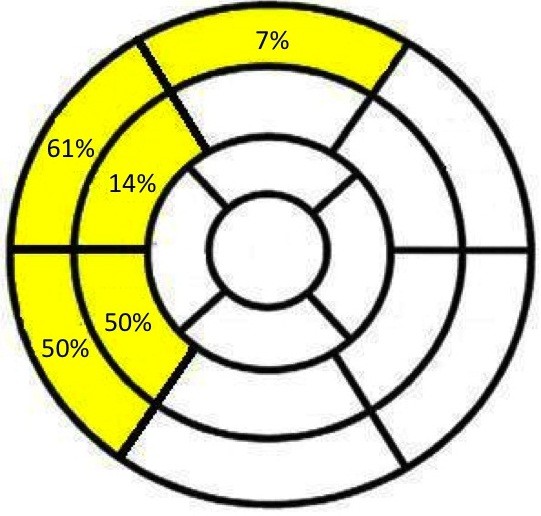
Results: Ninety-one patients (61 ± 21 years; 57 male) with aortic stenosis (aortic valve area 0.93 ± 0.32 cm2) were recruited. The severity of aortic stenosis was unrelated to the degree (r2=0.012, P=0.43) and pattern (P=0.22) of hypertrophy. By univariate analysis, only male sex demonstrated an association with LV mass index (P=0.02). Six patterns of LV adaption were observed: normal ventricular geometry (n=11), concentric remodeling (n=11), asymmetric remodeling (n=11), concentric hypertrophy (n=34), asymmetric hypertrophy (n=14) and LV decompensation (n=10). Asymmetric patterns displayed considerable overlap in appearances (wall thickness 17 ± 2mm) with hypertrophic cardiomyopathy.
Conclusions: We have demonstrated that in patients with moderate and severe aortic stenosis, the pattern of LV adaption and degree of hypertrophy do not closely correlate with the severity of valve narrowing and that asymmetric patterns of wall thickening are common.
Trial registration: ClinicalTrials.gov NCT00930735.
Figures


References
-
- Carabello BA. The relationship of left ventricular geometry and hypertrophy to left ventricular function in valvular heart disease. J Heart Valve Dis. 1995;4(Suppl 2):S132–S138. discussion S138–139. - PubMed
