

Gestational diabetes screening with the new IADPSG guidelines: a cost-effectiveness analysis
- PMID: 22840972
- PMCID: PMC4621259
- DOI: 10.1016/j.ajog.2012.06.048
Gestational diabetes screening with the new IADPSG guidelines: a cost-effectiveness analysis
Abstract
Objective: This study investigates the cost effectiveness of gestational diabetes mellitus screening using the new International Association of Diabetes in Pregnancy Study Group (IADPSG) guidelines.
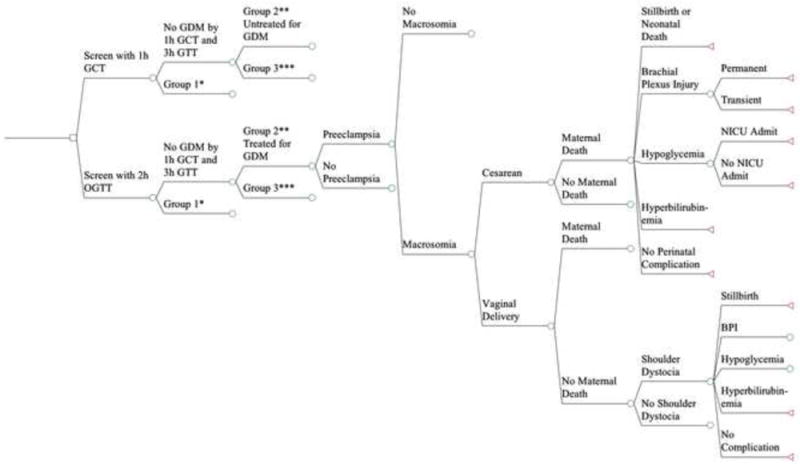
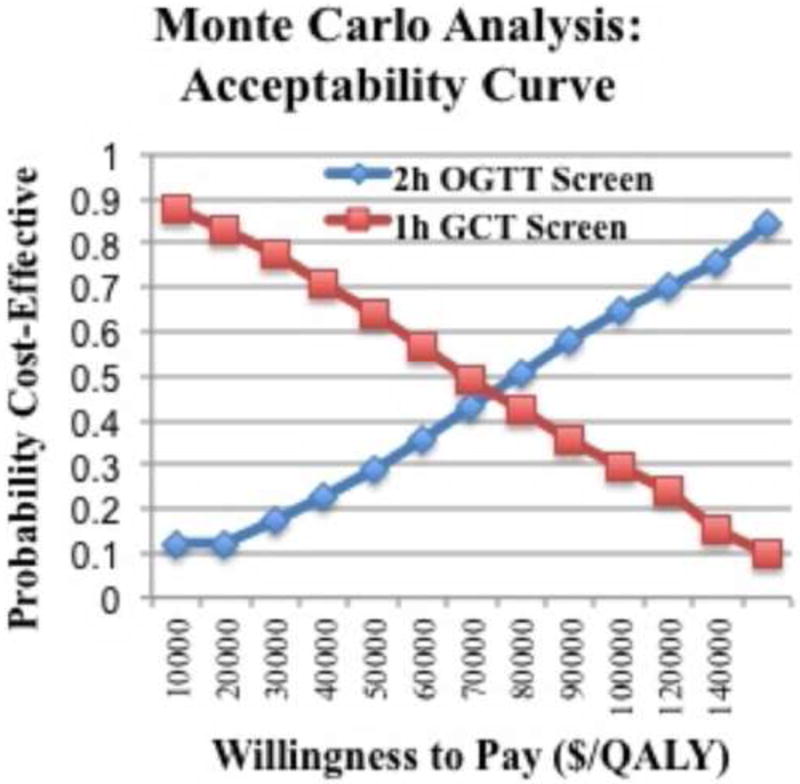
Study design: A decision analytic model was built comparing routine screening with the 2-hour (2h) oral glucose tolerance test (OGTT) vs the 1-hour glucose challenge test. All probabilities, costs, and benefits were derived from the literature. Base case, sensitivity analyses, and a Monte Carlo simulation were performed.
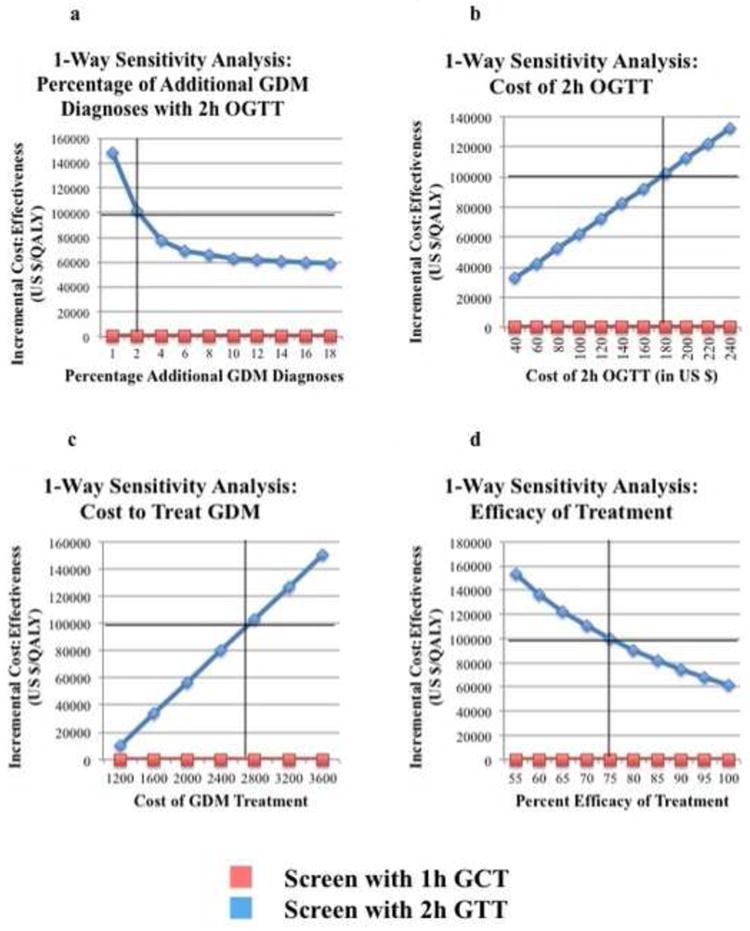
Results: Screening with the 2h OGTT was more expensive, more effective, and cost effective at $61,503/quality-adjusted life year. In a 1-way sensitivity analysis, the more inclusive IADPSG diagnostic approach remained cost effective as long as an additional 2.0% or more of patients were diagnosed and treated for gestational diabetes mellitus.
Conclusion: Screening at 24-28 weeks' gestational age under the new IADPSG guidelines with the 2h OGTT is expensive but cost effective in improving maternal and neonatal outcomes. How the health care system will provide expanded care to this group of women will need to be examined.
Copyright © 2012 Mosby, Inc. All rights reserved.
Conflict of interest statement
DISCLOSURE: None of the authors have a conflict of interest
Figures
Similar articles
-
Screening for gestational diabetes mellitus: are the criteria proposed by the international association of the Diabetes and Pregnancy Study Groups cost-effective?Diabetes Care. 2012 Mar;35(3):529-35. doi: 10.2337/dc11-1643. Epub 2012 Jan 20. Diabetes Care. 2012. PMID: 22266735 Free PMC article.
-
Cost-effectiveness of the New Zealand diabetes in pregnancy guideline screening recommendations.BMJ Open. 2015 Jun 22;5(6):e006996. doi: 10.1136/bmjopen-2014-006996. BMJ Open. 2015. PMID: 26100024 Free PMC article.
-
The impact of adoption of the international association of diabetes in pregnancy study group criteria for the screening and diagnosis of gestational diabetes.Am J Obstet Gynecol. 2015 Feb;212(2):224.e1-9. doi: 10.1016/j.ajog.2014.08.027. Epub 2014 Aug 27. Am J Obstet Gynecol. 2015. PMID: 25173183
-
Gestational diabetes guidelines in a HAPO world.Best Pract Res Clin Endocrinol Metab. 2010 Aug;24(4):673-85. doi: 10.1016/j.beem.2010.05.009. Best Pract Res Clin Endocrinol Metab. 2010. PMID: 20832745 Review.
-
NIH consensus development conference: diagnosing gestational diabetes mellitus.NIH Consens State Sci Statements. 2013 Mar 6;29(1):1-31. NIH Consens State Sci Statements. 2013. PMID: 23748438
Cited by
-
Changing diagnostic criteria for gestational diabetes in Sweden - a stepped wedge national cluster randomised controlled trial - the CDC4G study protocol.BMC Pregnancy Childbirth. 2019 Nov 1;19(1):398. doi: 10.1186/s12884-019-2547-5. BMC Pregnancy Childbirth. 2019. PMID: 31675922 Free PMC article.
-
A Review of the Associations Between Obstructive Sleep Apnea and Gestational Diabetes Mellitus and Possible Mechanisms of Disease.Reprod Sci. 2023 Jan;30(1):81-92. doi: 10.1007/s43032-022-00904-3. Epub 2022 Mar 7. Reprod Sci. 2023. PMID: 35257355 Free PMC article. Review.
-
Cost-effectiveness Analysis of Intraoperative Cell Salvage for Obstetric Hemorrhage.Anesthesiology. 2018 Feb;128(2):328-337. doi: 10.1097/ALN.0000000000001981. Anesthesiology. 2018. PMID: 29194062 Free PMC article.
-
Health economic modeling to assess short-term costs of maternal overweight, gestational diabetes, and related macrosomia - a pilot evaluation.Front Pharmacol. 2015 May 20;6:103. doi: 10.3389/fphar.2015.00103. eCollection 2015. Front Pharmacol. 2015. PMID: 26042038 Free PMC article.
-
Postdelivery Intervention to Prevent Type 2 Diabetes and the Cost-Effectiveness of Screening Criteria for Gestational Diabetes.Prev Chronic Dis. 2022 Dec 29;19:E89. doi: 10.5888/pcd19.220055. Prev Chronic Dis. 2022. PMID: 36580414 Free PMC article.
References
-
- Wier LM, Witt E, Burgess J, Elixhauser A. Healthcare Cost and Utilization Project (HCUP) Statistical Briefs. Rockville MD: 2006. Hospitalizations Related to Diabetes in Pregnancy, 2008: Statistical Brief #102. - PubMed
-
- Hillier TA, Vesco KK, Pedula KL, Beil TL, Whitlock EP, Pettitt DJ. Screening for gestational diabetes mellitus: a systematic review for the U.S. Preventive Services Task Force. Ann Intern Med. 2008;148:766–75. - PubMed
-
- Metzger BE, Lowe LP, Dyer AR, et al. Hyperglycemia and adverse pregnancy outcomes. N Engl J Med. 2008;358:1991–2002. - PubMed
-
- Landon MB, Gabbe SG. Gestational diabetes mellitus. Obstet Gynecol. 2011;118:1379–93. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
