

Temporary biventricular pacing decreases the vasoactive-inotropic score after cardiac surgery: a substudy of a randomized clinical trial
- PMID: 22841906
- PMCID: PMC3491102
- DOI: 10.1016/j.jtcvs.2012.07.020
Temporary biventricular pacing decreases the vasoactive-inotropic score after cardiac surgery: a substudy of a randomized clinical trial
Abstract
Objective: Vasoactive medications improve hemodynamics after cardiac surgery but are associated with high metabolic and arrhythmic burdens. The vasoactive-inotropic score was developed to quantify vasoactive and inotropic support after cardiac surgery in pediatric patients but may be useful in adults as well. Accordingly, we examined the time course of this score in a substudy of the Biventricular Pacing After Cardiac Surgery trial. We hypothesized that the score would be lower in patients randomized to biventricular pacing.
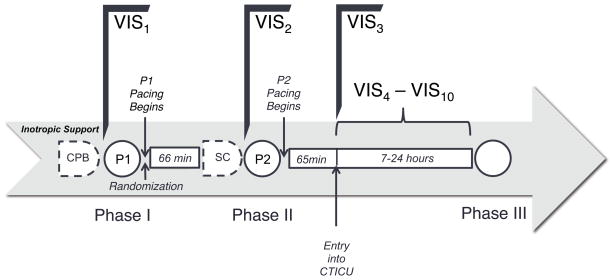
Methods: Fifty patients selected for increased risk of left ventricular dysfunction after cardiac surgery and randomized to temporary biventricular pacing or standard of care (no pacing) after cardiopulmonary bypass were studied in a clinical trial between April 2007 and June 2011. Vasoactive agents were assessed after cardiopulmonary bypass, after sternal closure, and 0 to 7 hours after admission to the intensive care unit.
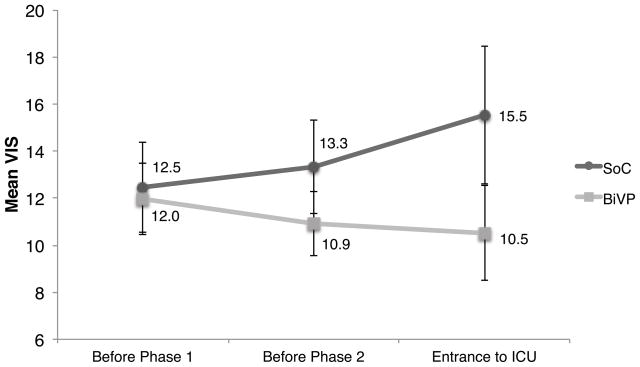
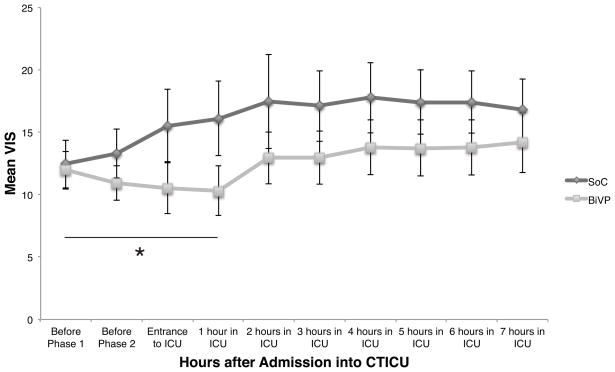
Results: Over the initial 3 collection points after cardiopulmonary bypass (mean duration, 131 minutes), the mean vasoactive-inotropic score decreased in the biventricular pacing group from 12.0 ± 1.5 to 10.5 ± 2.0 and increased in the standard of care group from 12.5 ± 1.9 to 15.5 ± 2.9. By using a linear mixed-effects model, the slopes of the time courses were significantly different (P = .02) and remained so for the first hour in the intensive care unit. However, the difference was no longer significant beyond this point (P = .26).
Conclusions: The vasoactive-inotropic score decreases in patients undergoing temporary biventricular pacing in the early postoperative period. Future studies are required to assess the impact of this effect on arrhythmogenesis, morbidity, mortality, and hospital costs.
Keywords: 16; 17; 21; 31; BiPACS; BiVP; Biventricular Pacing After Cardiac Surgery; CPB; ICU; MVO2; SOC; VIS; VIS(max); biventricular pacing; cardiopulmonary bypass; intensive care unit; maximum vasoactive-inotropic score; myocardial oxygen consumption; standard of care; vasoactive-inotropic score.
Copyright © 2013 The American Association for Thoracic Surgery. Published by Mosby, Inc. All rights reserved.
Figures
References
-
- Wernovsky G, Wypij D, Jonas RA, Mayer JE, Hanley FL, Hickey PR, et al. Postoperative course and hemodynamic profile after the arterial switch operation in neonates and infants. A comparison of low-flow cardiopulmonary bypass and circulatory arrest. Circulation. 1995;92(8):2226–2235. - PubMed
-
- Talwar S, Sandeep JA, Choudhary SK, Velayoudham D, Lakshmy R, Kasthuri JM, et al. Effect of preoperative administration of allopurinol in patients undergoing surgery for valvular heart diseases. Eur J Cardiothorac Surg. 2010;38(1):86–90. - PubMed
-
- Rhodes JF, Blaufox AD, Seiden HS, Asnes JD, Gross RP, Rhodes JP, et al. Cardiac arrest in infants after congenital heart surgery. Circulation. 1999;100(19 Suppl):II194–9. - PubMed
-
- Gruenwald CE, McCrindle BW, Crawford-Lean L, Holtby H, Parshuram C, Massicotte P, et al. Reconstituted fresh whole blood improves clinical outcomes compared with stored component blood therapy for neonates undergoing cardiopulmonary bypass for cardiac surgery: a randomized controlled trial. J Thorac Cardiovasc Surg. 2008;136(6):1442–1449. - PMC - PubMed
-
- Kulik TJ, Moler FW, Palmisano JM, Custer JR, Mosca RS, Bove EL, et al. Outcome-associated factors in pediatric patients treated with extracorporeal membrane oxygenator after cardiac surgery. Circulation. 1996;94(9 Suppl):II63–8. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
