

Tafamidis for transthyretin familial amyloid polyneuropathy: a randomized, controlled trial
- PMID: 22843282
- PMCID: PMC4098875
- DOI: 10.1212/WNL.0b013e3182661eb1
Tafamidis for transthyretin familial amyloid polyneuropathy: a randomized, controlled trial
Abstract
Objectives: To evaluate the efficacy and safety of 18 months of tafamidis treatment in patients with early-stage V30M transthyretin familial amyloid polyneuropathy (TTR-FAP).
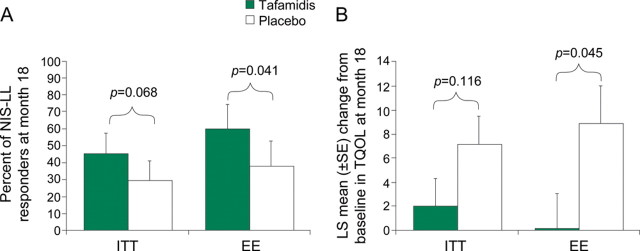
Methods: In this randomized, double-blind trial, patients received tafamidis 20 mg QD or placebo. Coprimary endpoints were the Neuropathy Impairment Score-Lower Limbs (NIS-LL) responder analysis (<2-point worsening) and treatment-group difference in the mean change from baseline in Norfolk Quality of Life-Diabetic Neuropathy total score (TQOL) in the intent-to-treat (ITT) population (n = 125). These endpoints were also evaluated in the efficacy-evaluable (EE; n = 87) population. Secondary endpoints, including changes in neurologic function, nutritional status, and TTR stabilization, were analyzed in the ITT population.
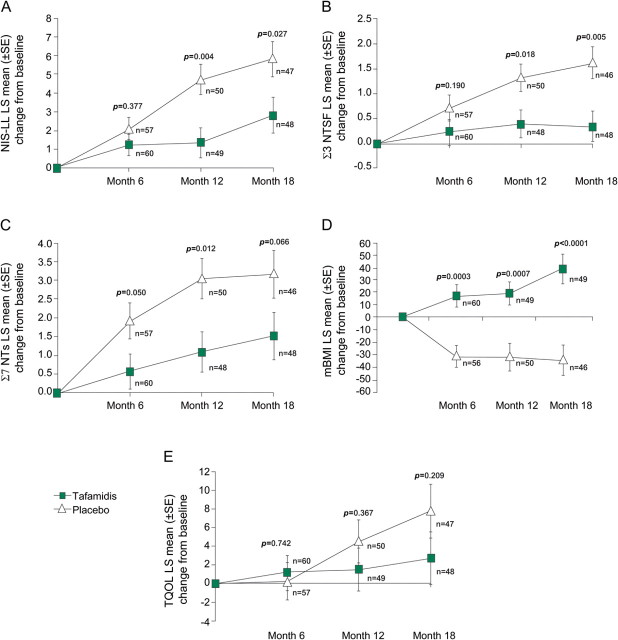
Results: There was a higher-than-anticipated liver transplantation dropout rate. No differences were observed between the tafamidis and placebo groups for the coprimary endpoints, NIS-LL responder analysis (45.3% vs 29.5% responders; p = 0.068) and change in TQOL (2.0 vs 7.2; p = 0.116) in the ITT population. In the EE population, significantly more tafamidis patients than placebo patients were NIS-LL responders (60.0% vs 38.1%; p = 0.041), and tafamidis patients had better-preserved TQOL (0.1 vs 8.9; p = 0.045). Significant differences in most secondary endpoints favored tafamidis. TTR was stabilized in 98% of tafamidis and 0% of placebo patients (p < 0.0001). Adverse events were similar between groups.
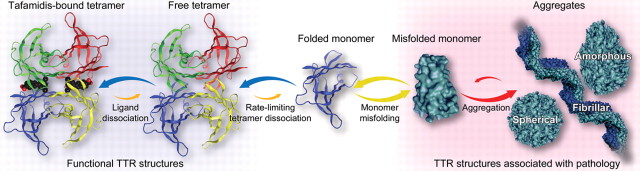
Conclusions: Although the coprimary endpoints were not met in the ITT population, tafamidis was associated with no trend toward more NIS-LL responders and a significant reduction in worsening of most neurologic variables, supporting the hypothesis that preventing TTR dissociation can delay peripheral neurologic impairment.
Classification of evidence: This study provides Class II evidence that 20 mg tafamidis QD was associated with no difference in clinical progression in patients with TTR-FAP, as measured by the NIS-LL and the Norfolk QOL-DN score. Secondary outcomes demonstrated a significant delay in peripheral neurologic impairment with tafamidis, which was well tolerated over 18 months.
Figures
Comment in
-
A designer drug for amyloid polyneuropathy.Neurology. 2012 Aug 21;79(8):730-1. doi: 10.1212/WNL.0b013e3182662041. Epub 2012 Jul 25. Neurology. 2012. PMID: 22843277 No abstract available.
-
Tafamidis for transthyretin familial amyloid polyneuropathy: a randomized, controlled trial.Neurology. 2013 Apr 9;80(15):1444-5. doi: 10.1212/01.wnl.0000429338.33391.87. Neurology. 2013. PMID: 23569001 No abstract available.
References
-
- Hund E, Linke RP, Willig F, Grau A. Transthyretin-associated neuropathic amyloidosis: pathogenesis and treatment. Neurology 2001;56:431–435. - PubMed
-
- Benson MD. The hereditary amyloidoses. Best Pract Res Clin Rheumatol 2003;17:909–927. - PubMed
-
- Planté-Bordeneuve V, Lalu T, Misrahi M, et al. Genotypic-phenotypic variations in a series of 65 patients with familial amyloid polyneuropathy. Neurology 1998;51:708–714. - PubMed
-
- Coutinho P, Martins da Silva A, Lopes Lima J, Resende Barbosa A. Forty years of experience with type I amyloid neuropathy: review of 483 cases. In: Glenner GG, Pinho e Costa P, Falcao de Freitas A. eds. Amyloid and Amyloidosis. Amsterdam: Excerpta Medica; 1980:88–98.
-
- Blake CC, Geisow MJ, Swan ID, Rerat C, Rerat B. Structure of human plasma prealbumin at 2.5 A resolution: a preliminary report on the polypeptide chain conformation, quaternary structure and thyroxine binding. J Mol Biol 1974;88:1–12. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous