

Augmented reality visualization with use of image overlay technology for MR imaging-guided interventions: assessment of performance in cadaveric shoulder and hip arthrography at 1.5 T
- PMID: 22843764
- PMCID: PMC3447176
- DOI: 10.1148/radiol.12112640
Augmented reality visualization with use of image overlay technology for MR imaging-guided interventions: assessment of performance in cadaveric shoulder and hip arthrography at 1.5 T
Abstract
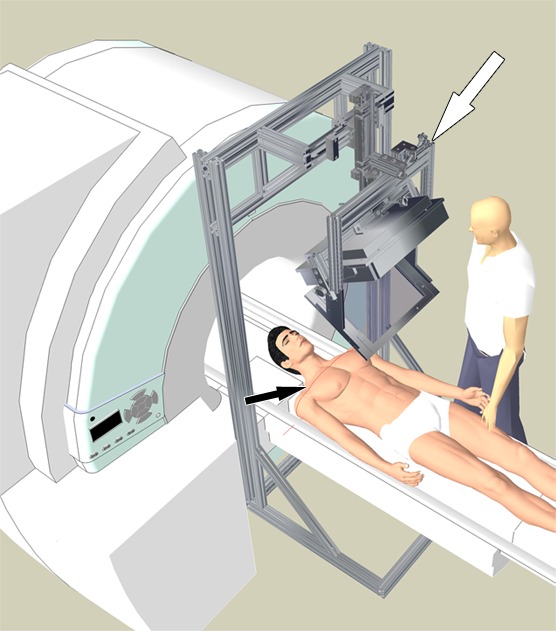
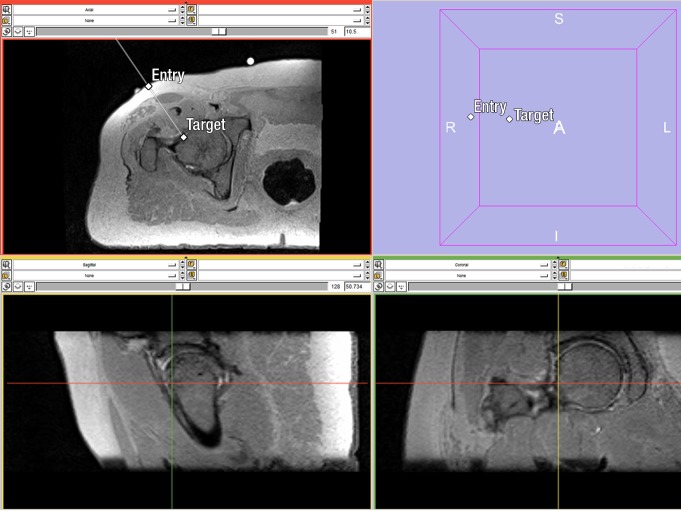
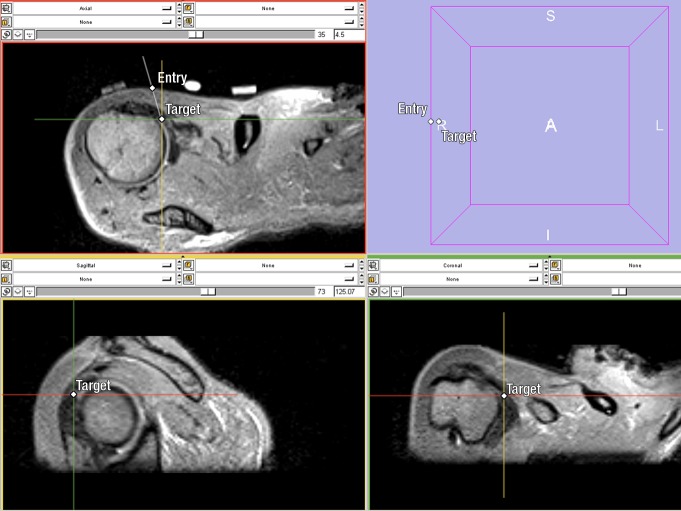
Purpose: To prospectively assess overlay technology in providing accurate and efficient targeting for magnetic resonance (MR) imaging-guided shoulder and hip joint arthrography.
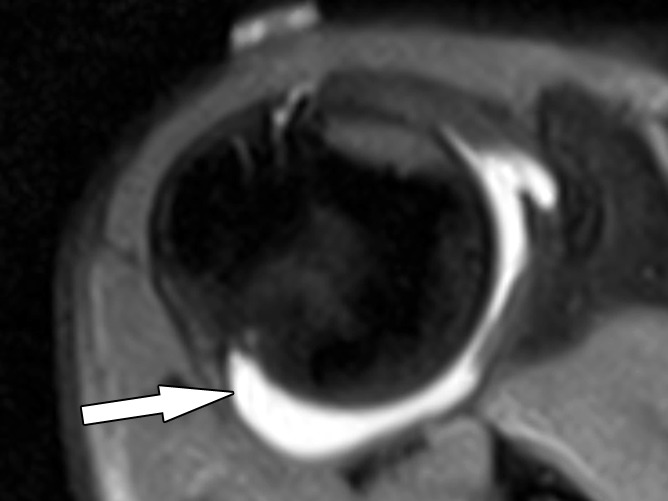
Materials and methods: A prototype augmented reality image overlay system was used in conjunction with a clinical 1.5-T MR imager. A total of 24 shoulder joint and 24 hip joint injections were planned in 12 human cadavers. Two operators (A and B) participated, each performing procedures on different cadavers using image overlay guidance. MR imaging was used to confirm needle positions, monitor injections, and perform MR arthrography. Accuracy was assessed according to the rate of needle adjustment, target error, and whether the injection was intraarticular. Efficiency was assessed according to arthrography procedural time. Operator differences were assessed with comparison of accuracy and procedure times between the operators. Mann-Whitney U test and Fisher exact test were used to assess group differences.
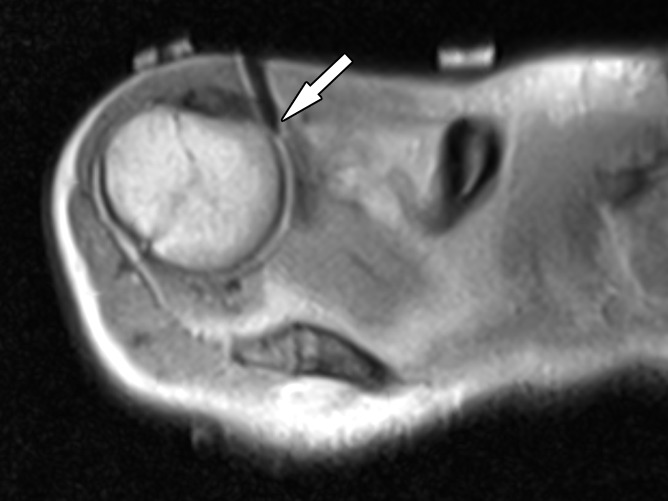
Results: Forty-five arthrography procedures (23 shoulders, 22 hips) were performed. Three joints had prostheses and were excluded. Operator A performed 12 shoulder and 12 hip injections. Operator B performed 11 shoulder and 10 hip injections. Needle adjustment rate was 13% (six of 45; one for operator A and five for operator B). Target error was 3.1 mm±1.2 (standard deviation) (operator A, 2.9 mm±1.4; operator B, 3.5 mm±0.9). Intraarticular injection rate was 100% (45 of 45). The average arthrography time was 14 minutes (range, 6-27 minutes; 12 minutes [range, 6-25 minutes] for operator A and 16 minutes [range, 6-27 min] for operator B). Operator differences were not significant with regard to needle adjustment rate (P=.08), target error (P=.07), intraarticular injection rate (P>.99), and arthrography time (P=.22).
Conclusion: Image overlay technology provides accurate and efficient MR guidance for successful shoulder and hip arthrography in human cadavers.
© RSNA, 2012.
Figures

References
-
- Miller TT. MR arthrography of the shoulder and hip after fluoroscopic landmarking. Skeletal Radiol 2000;29(2):81–84 - PubMed
-
- Mulligan ME. CT-guided shoulder arthrography at the rotator cuff interval. AJR Am J Roentgenol 2008;191(2):W58–W61 - PubMed
-
- Dépelteau H, Bureau NJ, Cardinal E, Aubin B, Brassard P. Arthrography of the shoulder: a simple fluoroscopically guided approach for targeting the rotator cuff interval. AJR Am J Roentgenol 2004;182(2):329–332 - PubMed
-
- Steinbach LS, Palmer WE, Schweitzer ME. Special focus session: MR arthrography. RadioGraphics 2002;22(5):1223–1246 - PubMed
-
- Nawfel RD, Judy PF, Silverman SG, Hooton S, Tuncali K, Adams DF. Patient and personnel exposure during CT fluoroscopy-guided interventional procedures. Radiology 2000;216(1):180–184 - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
