

Applications of transrectal ultrasound in prostate cancer
- PMID: 22844031
- PMCID: PMC3746408
- DOI: 10.1259/bjr/56357549
Applications of transrectal ultrasound in prostate cancer
Abstract
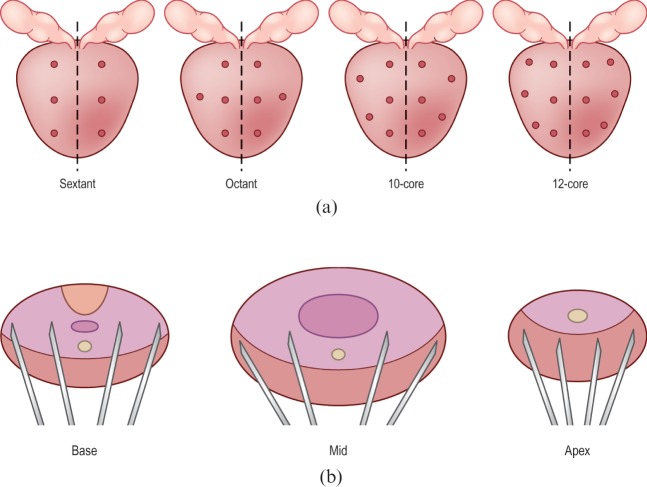
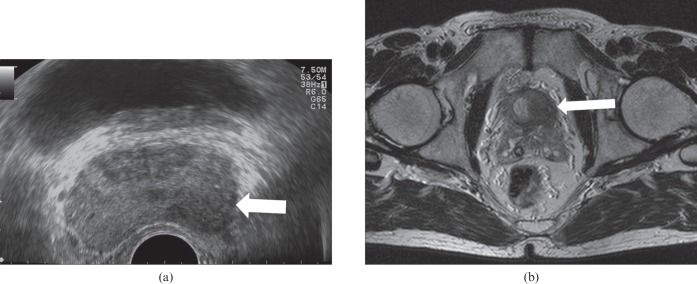
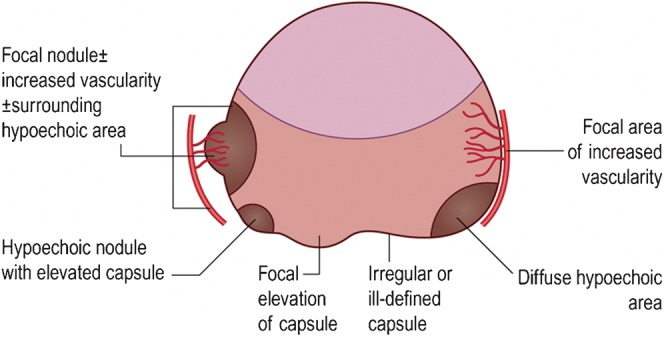
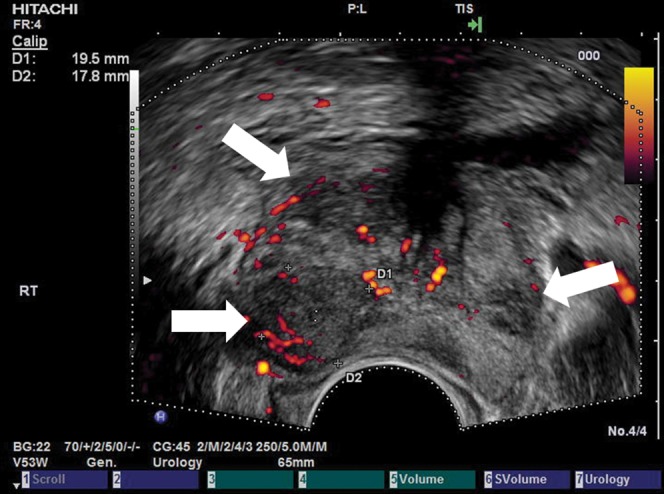
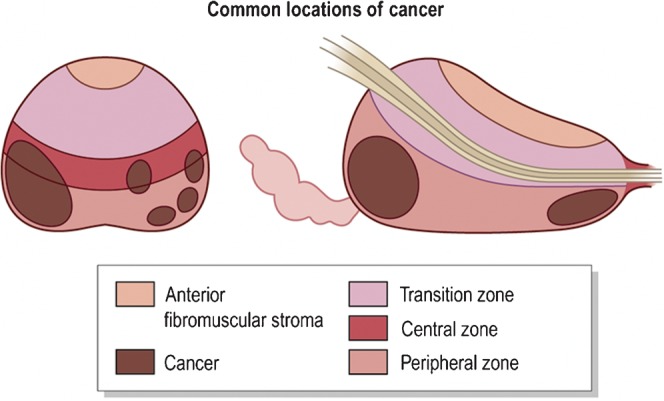
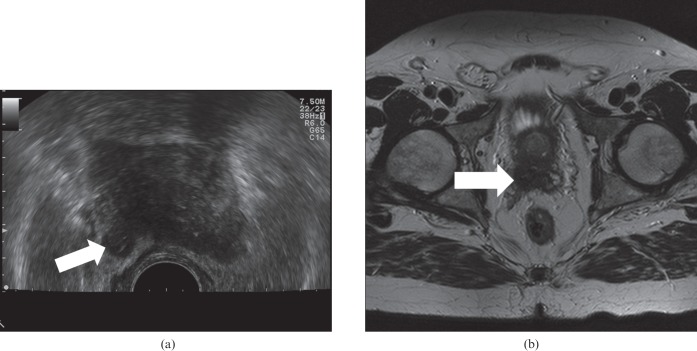
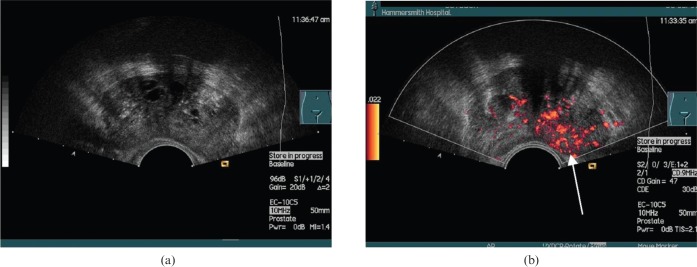
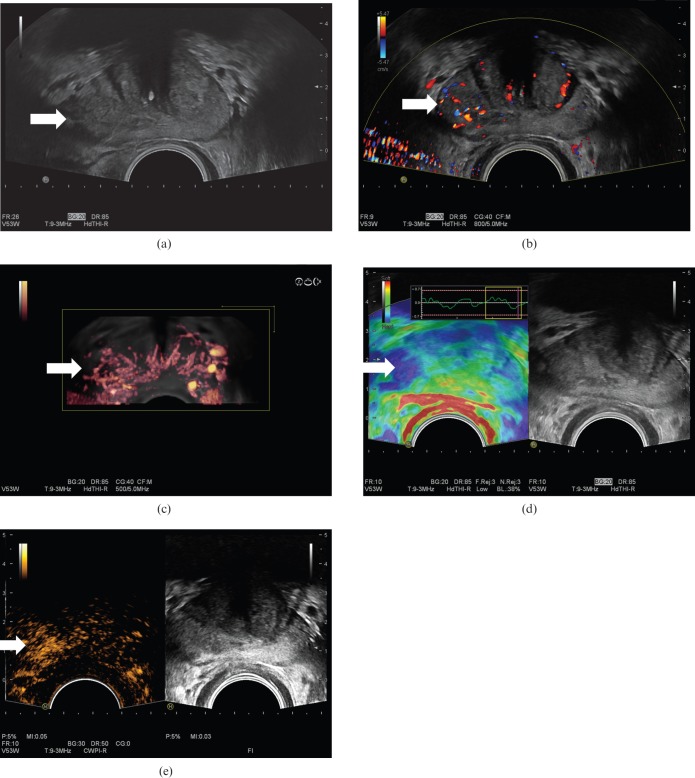
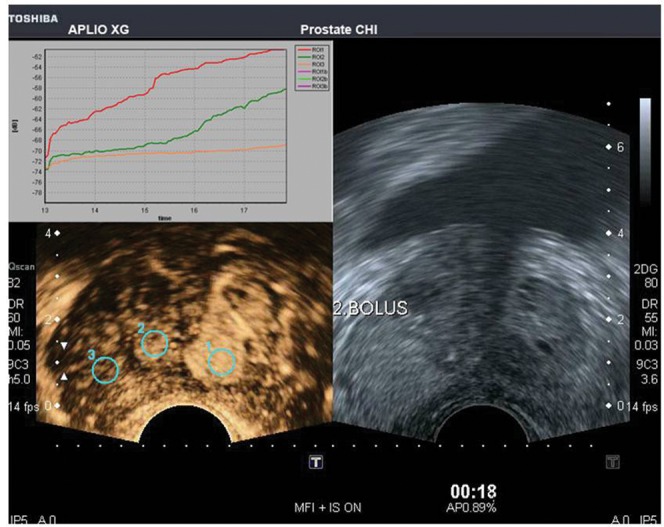
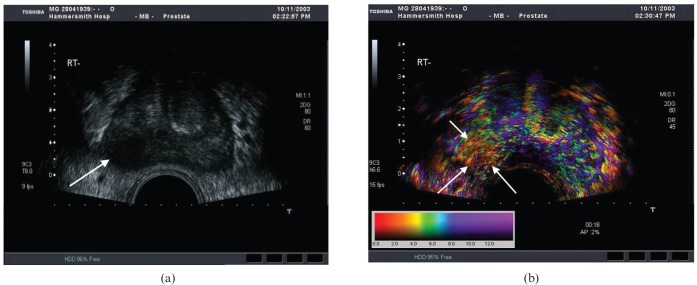
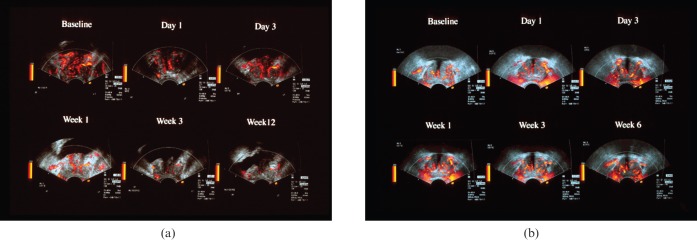
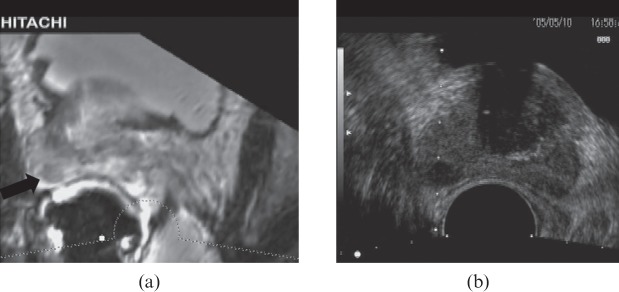
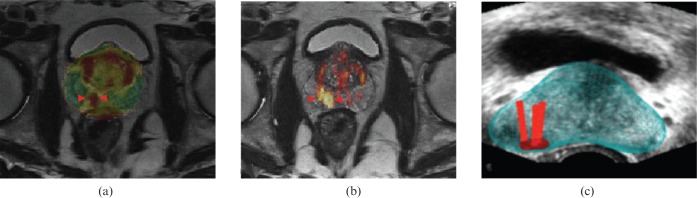
Transrectal ultrasound (TRUS) was first developed in the 1970s. TRUS-guided biopsy, under local anaesthetic and prophylactic antibiotics, is now the most widely accepted method to diagnose prostate cancer. However, the sensitivity and specificity of greyscale TRUS in the detection of prostate cancer is low. Prostate cancer most commonly appears as a hypoechoic focal lesion in the peripheral zone on TRUS but the appearances are variable with considerable overlap with benign lesions. Because of the low accuracy of greyscale TRUS, TRUS-guided biopsies have become established in the acquisition of systematic biopsies from standard locations. The number of systematic biopsies has increased over the years, with 10-12 cores currently accepted as the minimum standard. This article describes the technique of TRUS and biopsy and its complications. Novel modalities including contrast-enhanced modes and elastography as well as fusion techniques for increasing the sensitivity of TRUS-guided prostate-targeted biopsies are discussed along with their role in the diagnosis and management of prostate cancer.
Figures
References
-
- Northern Ireland Cancer Registry Cancer incidence and mortality. Belfast, UK: NICR; 2010
-
- Welsh Cancer Intelligence and Surveillance Unit Cardiff, UK: WCISU; 2010
-
- ISD Online Information and Statistics Division, NHS Scotland Edinburgh, UK: ISD Scotland; 2010
-
- Office for National Statistics Registrations of cancer diagnosed in 2008, England. Series MB1 no. 39. London, UK: National Statistics; 2010
-
- Sakr WA, Grignon DJ, Haas GP, Heilbrun LK, Pontes JE, Crissman JD. Age and racial distribution of prostatic intraepithelial neoplasia. Eur Urol 1996;30:138–44 - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
