

Evaluation of solitary pulmonary nodule detected during computed tomography examination
- PMID: 22844306
- PMCID: PMC3403798
- DOI: 10.12659/pjr.882967
Evaluation of solitary pulmonary nodule detected during computed tomography examination
Abstract
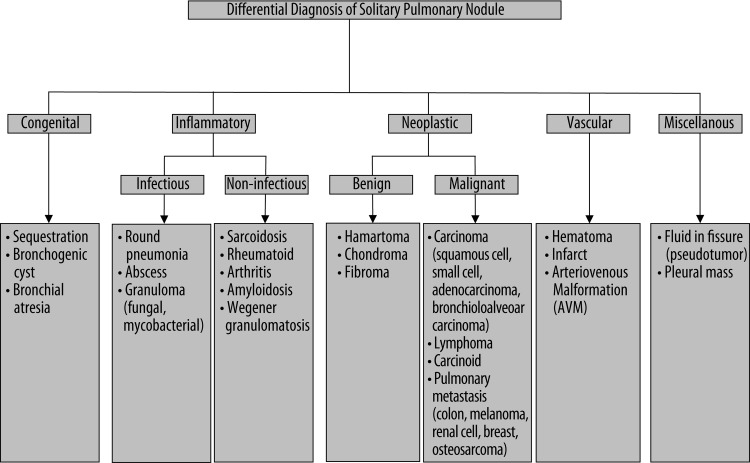
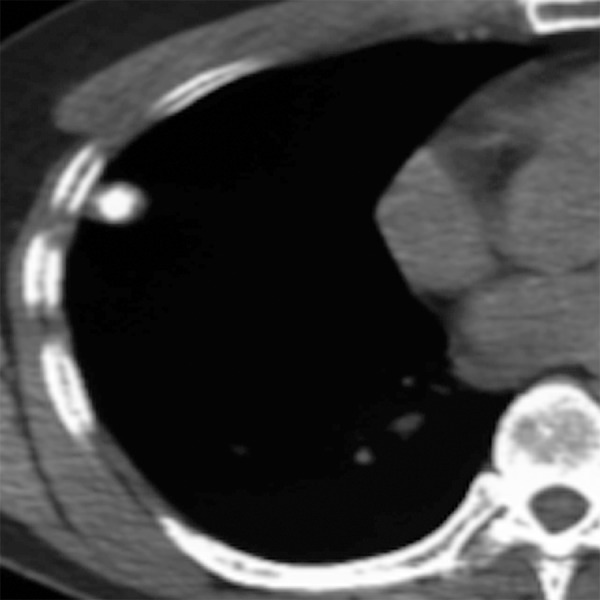
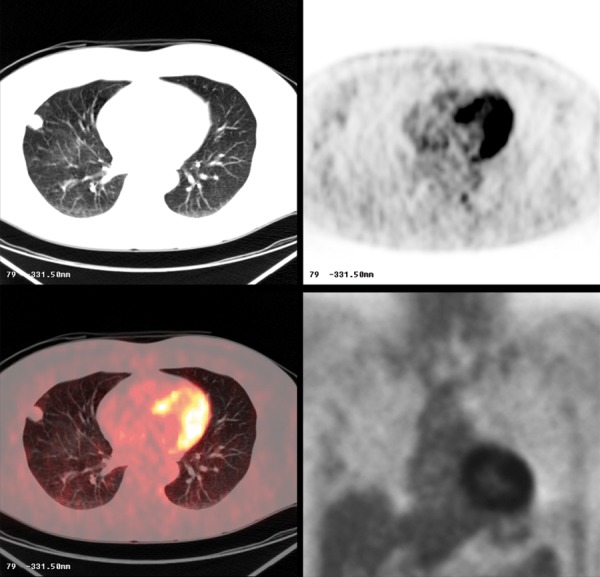
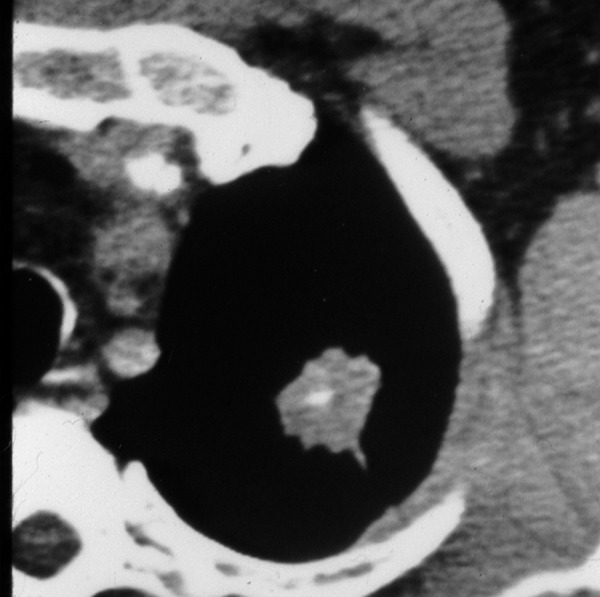
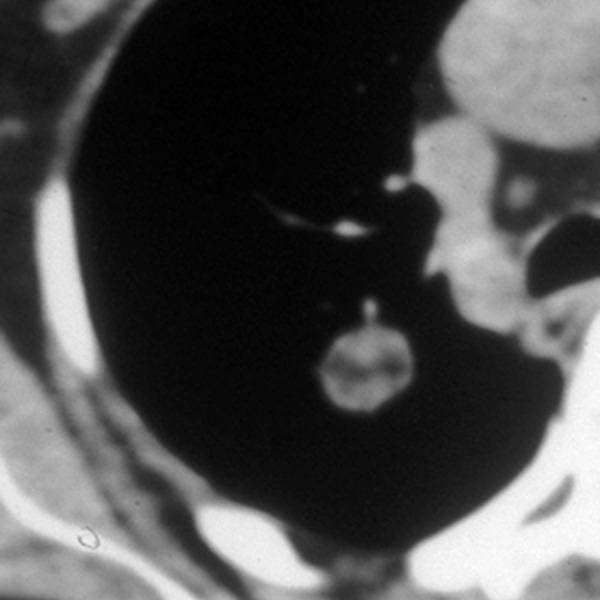
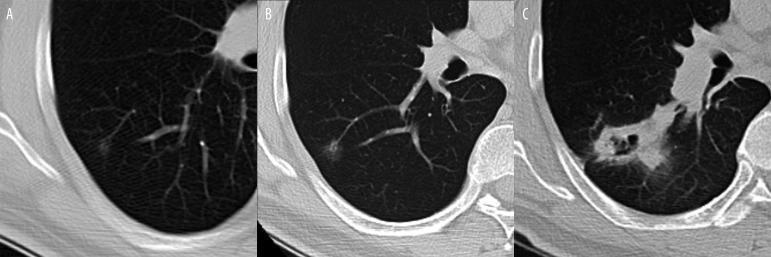
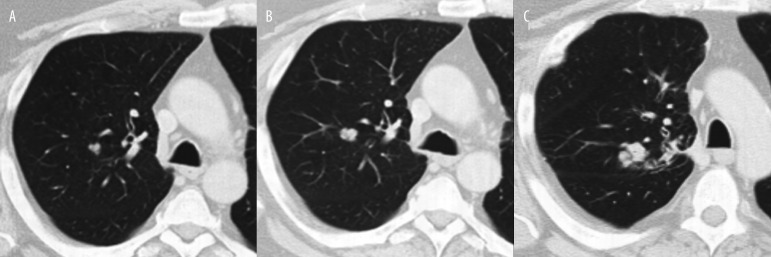
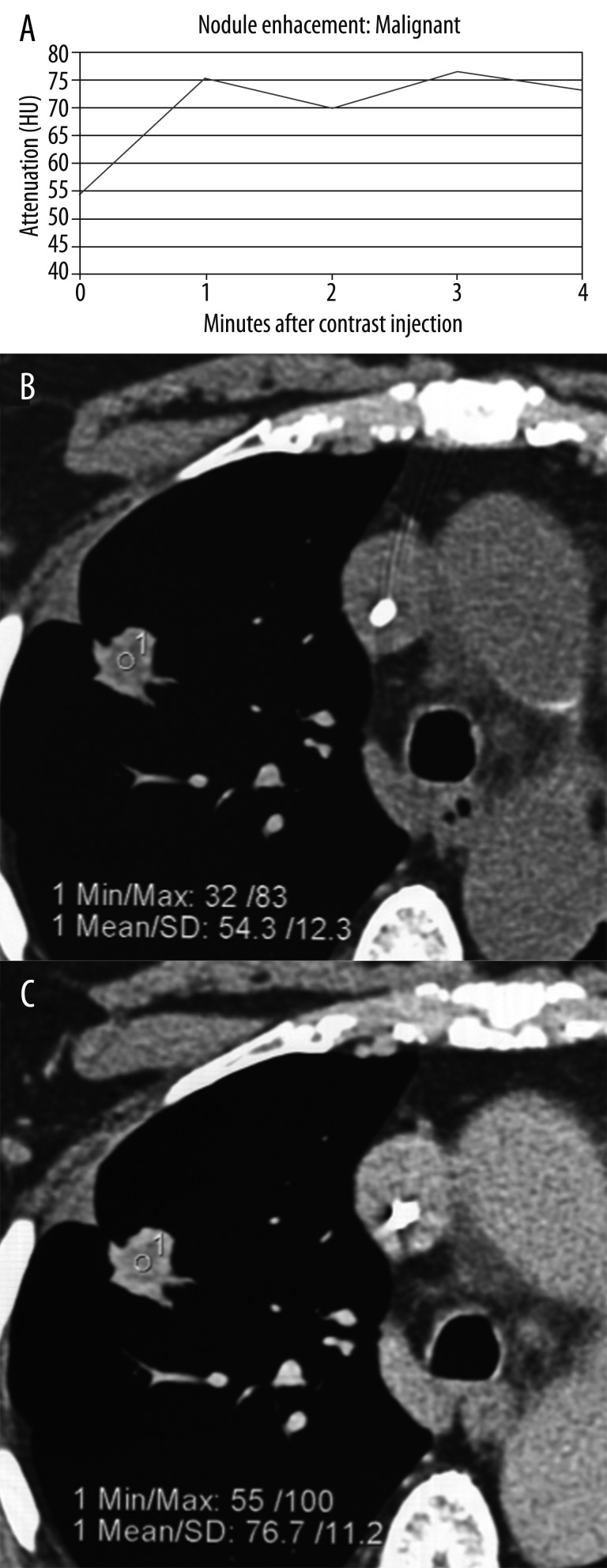
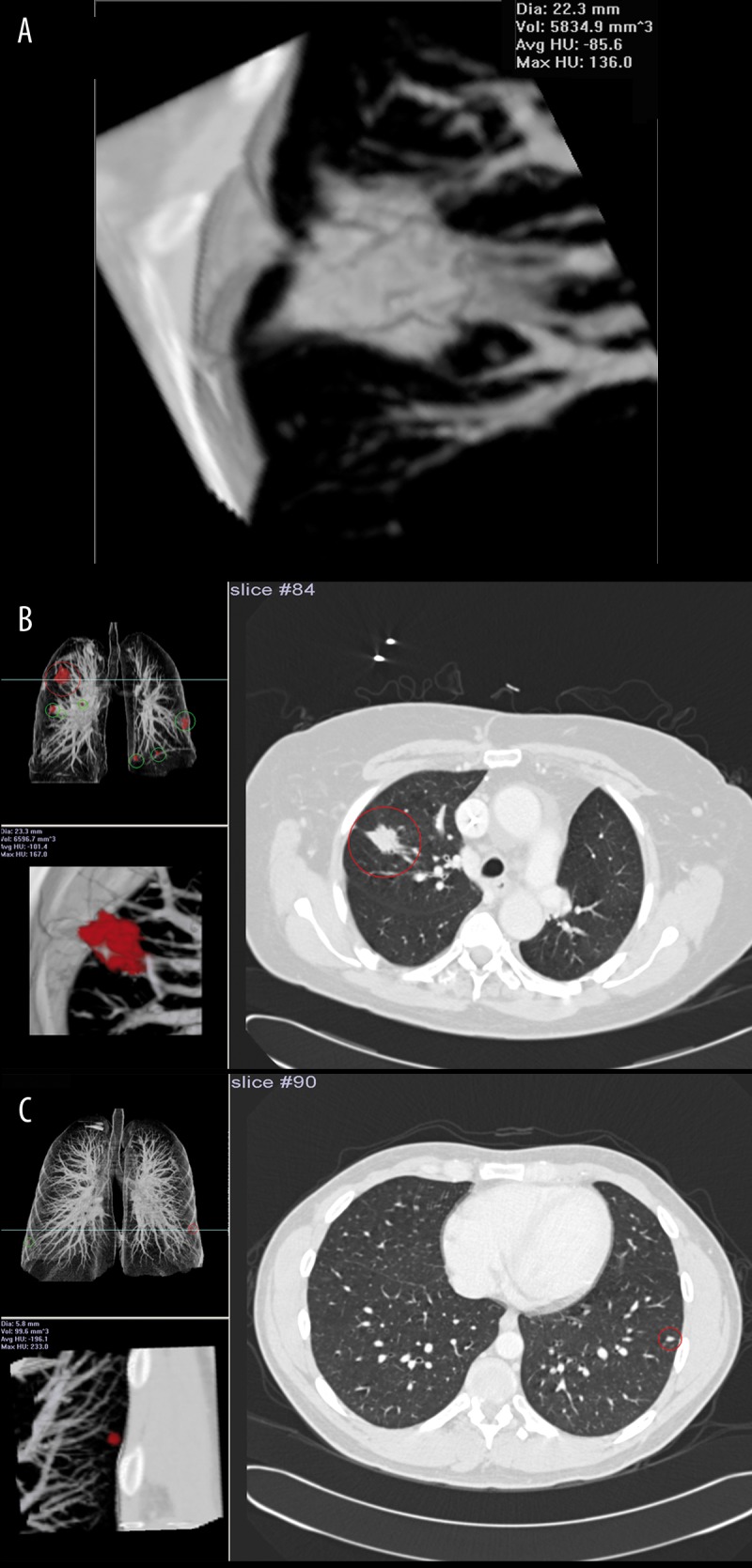
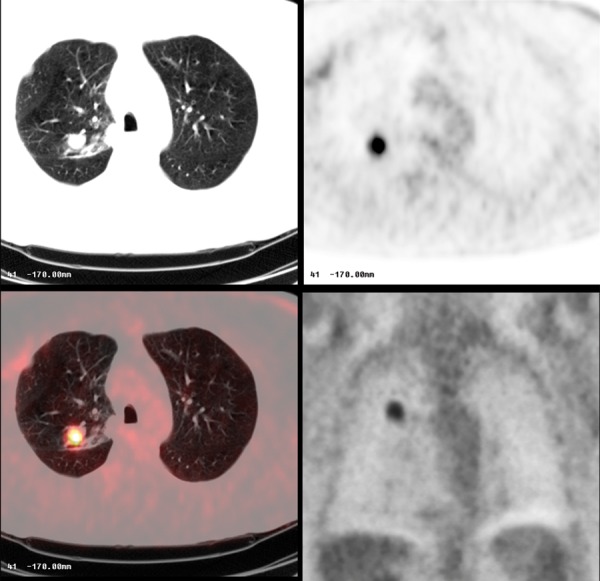
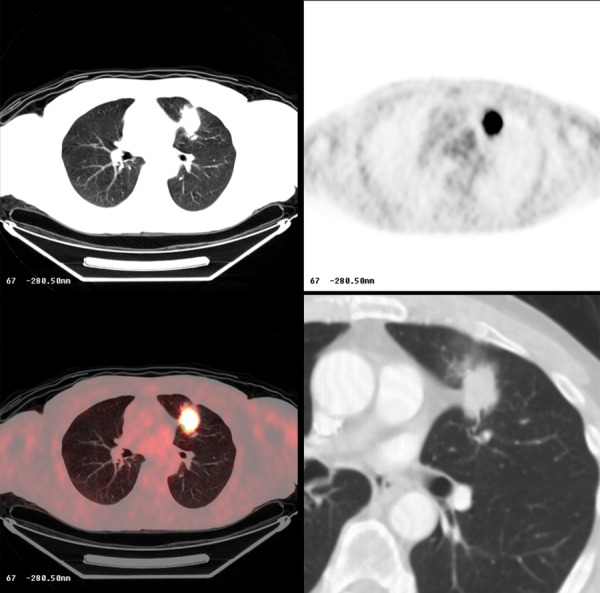
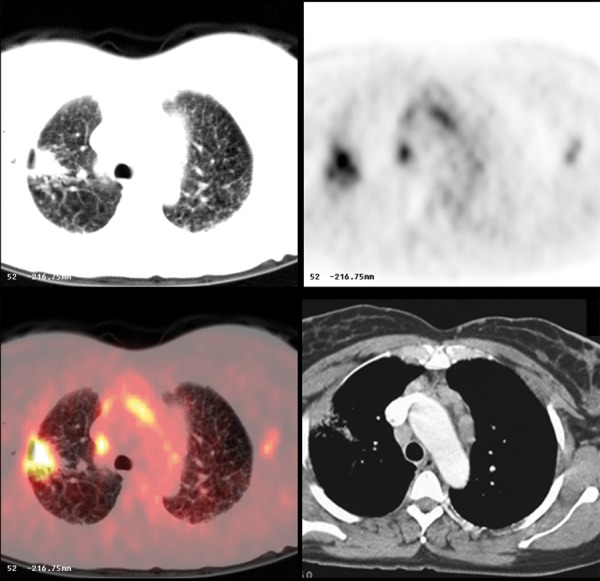
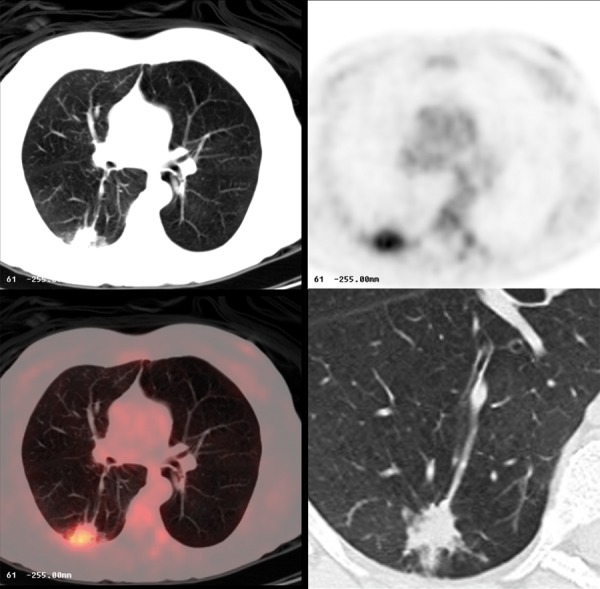
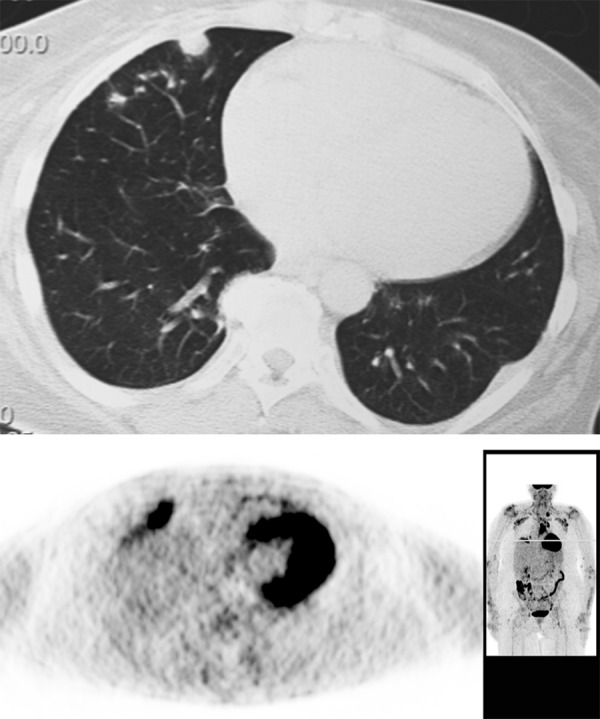
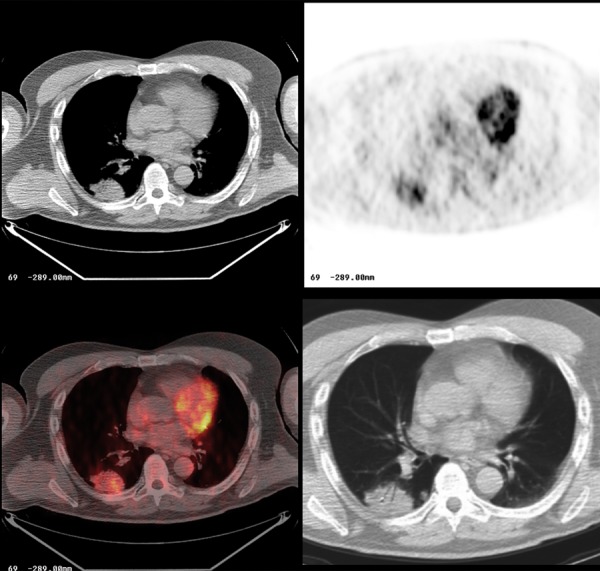
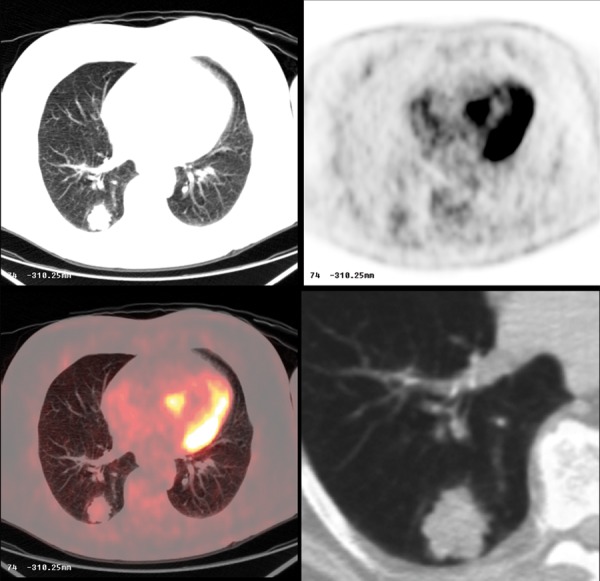
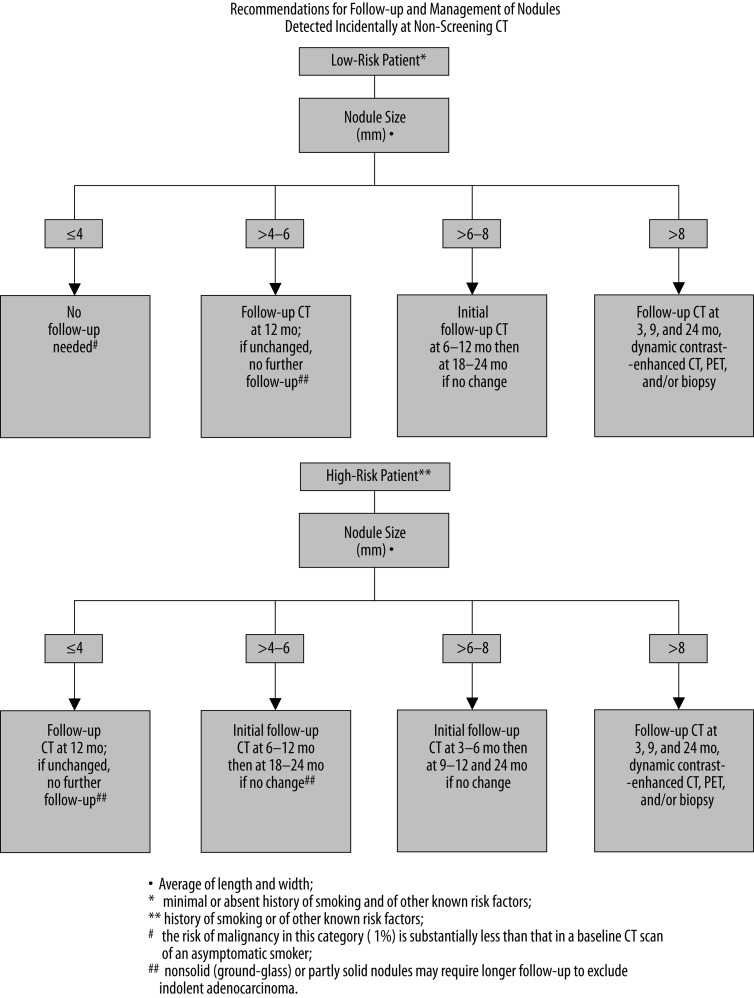
The solitary pulmonary nodule (SPN) has always been a diagnostic challenge for the radiologists. Currently, with increased utilization of computed tomography (CT) greater number of nodules is being discovered, with numerous indeterminate lesions, which frequently cannot be immediately classified into benign or malignant category.In this article we review the imaging features of benign and malignant round opacities; we demonstrate currently used standards and also more advanced techniques that are helpful in evaluating SPNs such as contrast-enhanced CT, PET/CT imaging and also pathologic sampling with biopsy or surgical resection.We also summarize the methods of evaluating and managing SPNs based on the latest guidelines from the Fleischner Society and American College of Chest Physicians.
Keywords: indeterminate nodule; multi-detector computed tomography (MDCT); solitary pulmonary nodule (SPN); transthoracic needle biopsy (TNB).
Figures


References
-
- Austin JH, Muller NL, Friedman PJ, et al. Glossary of terms for CT of the lungs: Recommendations of the nomenclature committee of the Fleischner Society. Radiology. 1996;200:327–31. - PubMed
-
- Gould MK, Fletcher J, Iannettoni MD, et al. American College of Chest Physician. Evaluation of patients with pulmonary nodules: when is it lung cancer?: ACCP evidence-based clinical practice guidelines (2nd edition) Chest. 2007;132(Suppl.3):108S–30S. - PubMed
-
- Erasmus JJ, Connolly JE, McAdams HP, et al. Solitary pulmonary nodules: Part I. Morphologic evaluation for differentiation of benign and malignant lesions. Radiographics. 2000;20:43–58. - PubMed
-
- Brandman S, Ko JP. Pulmonary nodule detection, characterization, and management with multidetector computed tomography. J Thorac Imaging. 2011;26(2):90–105. - PubMed
-
- Nicholas E, Braff S, Klein JS. Evaluation of the solitary pulmonary nodule: A practical approach. Applied Radiology. http://www.appliedradiology.com/Issues/2011/12/Articles/AR_12-11_Klein-N... (December 2011; vol.40, number 12) (accessed 29.04.2012)
LinkOut - more resources
Full Text Sources