

Which interventions offer best value for money in primary prevention of cardiovascular disease?
- PMID: 22844529
- PMCID: PMC3402472
- DOI: 10.1371/journal.pone.0041842
Which interventions offer best value for money in primary prevention of cardiovascular disease?
Abstract
Background: Despite many decades of declining mortality rates in the Western world, cardiovascular disease remains the leading cause of death worldwide. In this research we evaluate the optimal mix of lifestyle, pharmaceutical and population-wide interventions for primary prevention of cardiovascular disease.
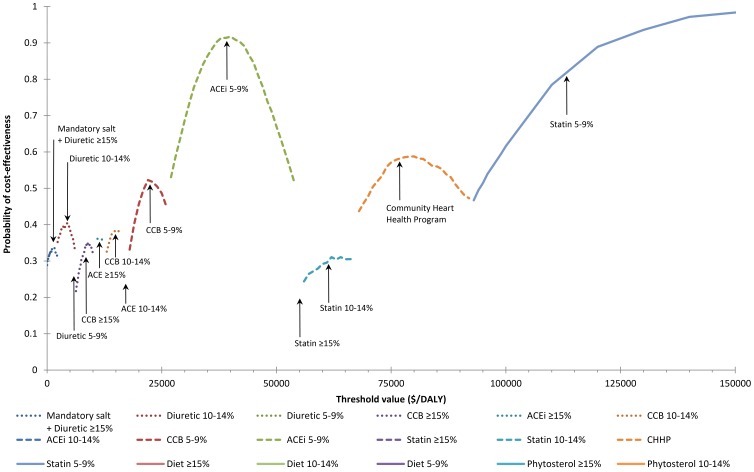
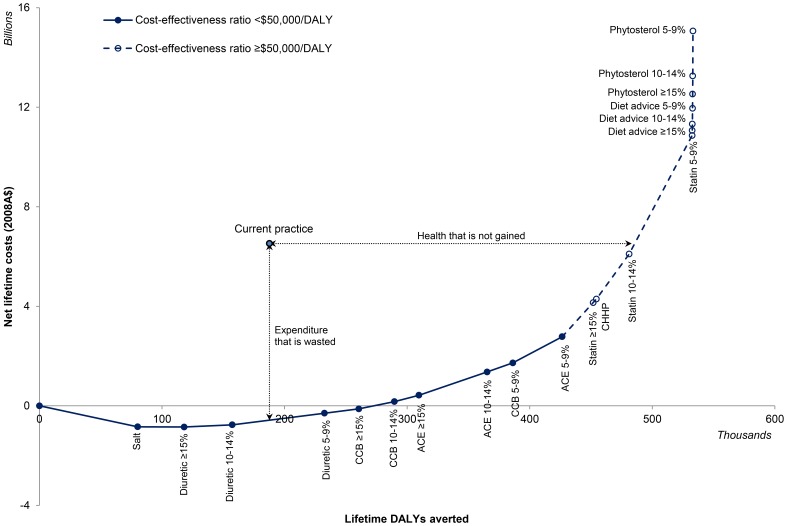
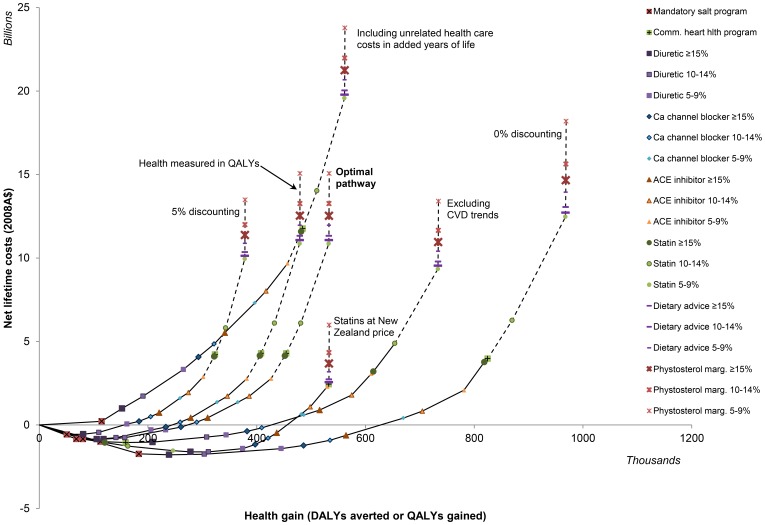
Methods and findings: In a discrete time Markov model we simulate the ischaemic heart disease and stroke outcomes and cost impacts of intervention over the lifetime of all Australian men and women, aged 35 to 84 years, who have never experienced a heart disease or stroke event. Best value for money is achieved by mandating moderate limits on salt in the manufacture of bread, margarine and cereal. A combination of diuretic, calcium channel blocker, ACE inhibitor and low-cost statin, for everyone with at least 5% five-year risk of cardiovascular disease, is also cost-effective, but lifestyle interventions aiming to change risky dietary and exercise behaviours are extremely poor value for money and have little population health benefit.
Conclusions: There is huge potential for improving efficiency in cardiovascular disease prevention in Australia. A tougher approach from Government to mandating limits on salt in processed foods and reducing excessive statin prices, and a shift away from lifestyle counselling to more efficient absolute risk-based prescription of preventive drugs, could cut health care costs while improving population health.
Conflict of interest statement
Figures
References
-
- Ford ES, Capewell S. Proportion of the Decline in Cardiovascular Mortality Disease due to Prevention Versus Treatment: Public Health Versus Clinical Care. Annual Review of Public Health. 2011;32:5–22. - PubMed
-
- Unal B, Critchley JA, Capewell S. Explaining the Decline in Coronary Heart Disease Mortality in England and Wales Between 1981 and 2000. Circulation. 2004;109:1101–1107. - PubMed
-
- WHO. The global burden of disease: 2004 update. Geneva: World Health Organization. 2008.
-
- Unal B, Critchley JA, Capewell S. Small changes in United Kingdom cardiovascular risk factors could halve coronary heart disease mortality. Journal of Clinical Epidemiology. 2005;58:733–740. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Miscellaneous
