

Intraoperative imprint cytology and frozen section pathology for margin assessment in breast conservation surgery: a systematic review
- PMID: 22847119
- PMCID: PMC4247998
- DOI: 10.1245/s10434-012-2492-2
Intraoperative imprint cytology and frozen section pathology for margin assessment in breast conservation surgery: a systematic review
Abstract
Background: Achieving negative surgical margins is critical to minimizing the risk of tumor recurrence in patients undergoing breast conservation surgery (BCS) for a breast malignancy. Our objective was to perform a systematic review comparing reexcision rates, sensitivity and specificity of the intraoperative use of the margin assessment techniques of imprint cytology (IC) and frozen section analysis (FSA), against permanent histopathologic section (PS).
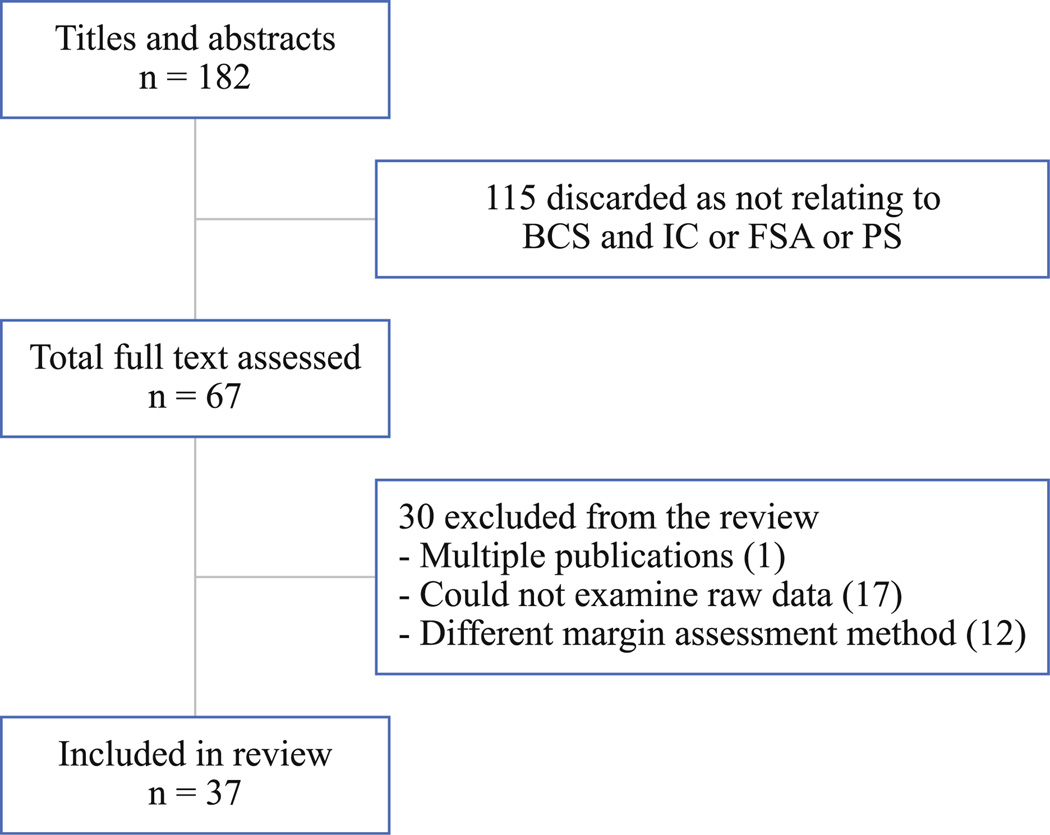
Methods: The databases PubMed, Web of Knowledge, Cochrane Library and CINAHL Plus were searched for literature published from 1997 to 2011. Original investigations of patients who underwent BCS for breast cancer that evaluated margin assessment with PS and/or IC or FSA were included. Of 182 titles identified, 41 patient cohorts from 37 articles met inclusion criteria: PS (n = 19), IC (n = 7) and FSA (n = 15). Studies were summarized qualitatively using the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) checklist for cohort studies and the Strength of Recommendation Taxonomy (SORT) numerical scale for diagnostic studies.
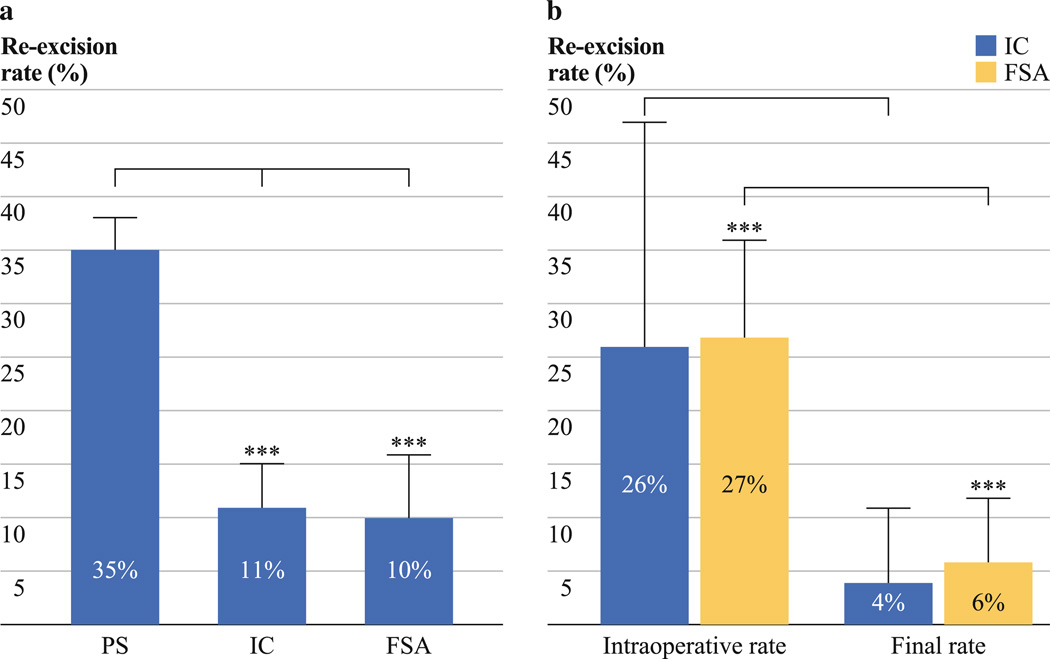
Results: The final reexcision rates after primary BCS were 35 % for PS, 11 % for IC (p = 0.001 vs. PS) and 10 % for FSA (p < 0.0001 vs. PS). For IC, reexcision rates decreased from 26 to 4 % (p = 0.18) and for FSA, reexcision rates decreased from 27 to 6 % (p < 0.0001). The pooled sensitivity of IC and FSA were 72 and 83 %. The pooled specificity of IC and FSA were 97 and 95 %. The average length of each technique was 13 min for IC and 27 min for FSA.
Conclusions: Patients who underwent BCS with intraoperative IC or FSA to assess negative surgical margins had significantly fewer secondary surgical procedures for excision of their breast malignancies.
Figures
References
-
- National Institutes of Health Consensus Conference. Treatment of early-stage breast cancer. JAMA. 1991;265:391–395. - PubMed
-
- Singletary SE. Surgical margins in patients with early-stage breast cancer treated with breast conservation therapy. Am J Surg. 2002;184:383–393. - PubMed
-
- Sabel MS. Surgical considerations in early-stage breast cancer: lessons learned and future directions. Semin Radiat Oncol. 2011;21:10–19. - PubMed
-
- Vapiwala N, Harris E, Huang WT, et al. Long-term outcome for mammographically detected ductal carcinoma in situ managed with breast conservation treatment: prognostic significance of reexcision. Cancer J. 2006;12:25–32. - PubMed
-
- Aziz D, Rawlinson E, Narod SA, et al. The role of reexcision for positive margins in optimizing local disease control after breast conserving surgery for cancer. Breast J. 2006;12:331–337. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
