

Clinical parameters for prediction of successful labor induction after application of intravaginal dinoprostone in nulliparous Chinese women
- PMID: 22847202
- PMCID: PMC3560701
- DOI: 10.12659/msm.883273
Clinical parameters for prediction of successful labor induction after application of intravaginal dinoprostone in nulliparous Chinese women
Abstract
Background: The aim of this study was to compare the possible clinical parameters for prediction of successful labor induction in Chinese nulliparous women.
Material/methods: A retrospective, observational trial of labor induction was performed, using a single dose of 10 mg controlled-release dinoprostone for preinduction cervical ripening in 127 nulliparous women (gestational age 38-42 weeks, singleton cephalic presentation). The characteristics of the women with successful labor induction (defined as vaginal delivery achieved on the day of admission; n=80) and failed labor induction (n=47) were compared.
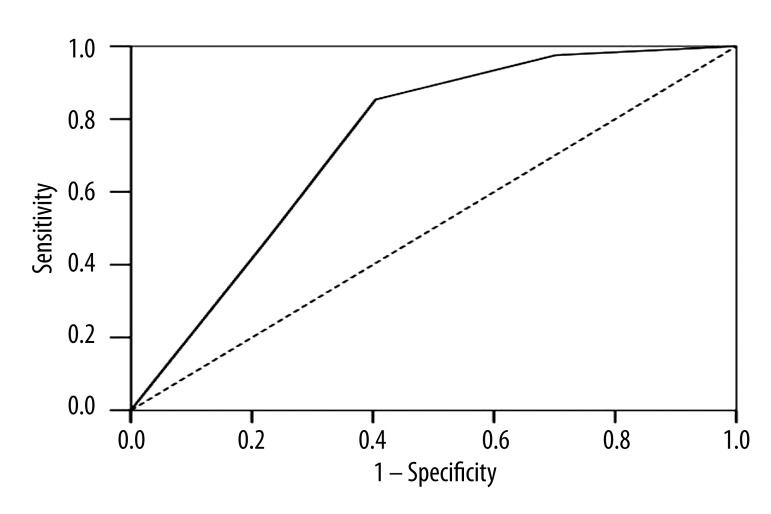
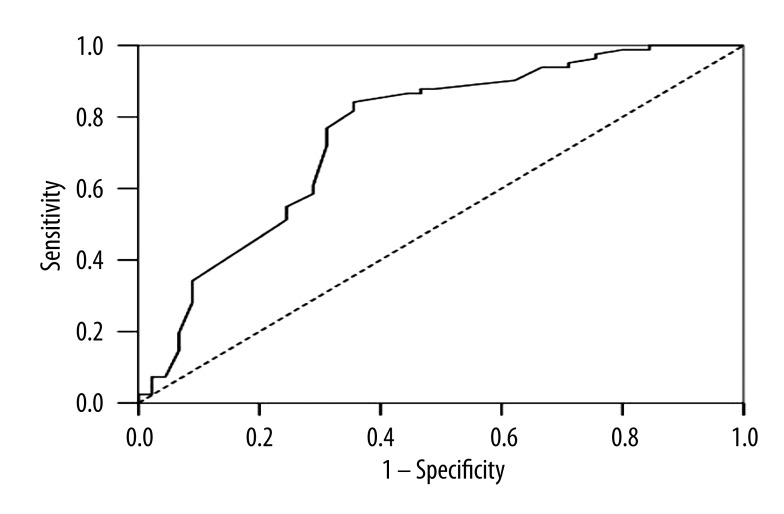
Results: The main differences observed between the groups were gravidity (P<0.05), induction-active labor interval (5.16±2.98 vs. 8.40±3.41; P<0.05) and birth weight (3421.11±368.14 vs. 3566.36±345.16; P<0.05). Logistic regression demonstrated that gravidity (P<0.05) and induction-active labor interval (P<0.05), but not Bishop score, were significant and independent contributing factors for successful labor induction. In the receiver operating characteristic curves for the prediction of successful labor induction, the best cut-off value for gravidity was 3 (95% confidence interval [CI] 0.64-0.83, P=0.000), and the best cut-off value for the induction-active labor interval was 7.96 (95%CI 0.66-0.85, P=0.000).
Conclusions: Less gravidity and shorter induction-active labor interval predict successful labor induction with reasonable accuracy.
Figures
References
-
- Lilford RJ, van Coeverden de Groot HA, et al. The relative risks of caesarean section (intrapartum and elective) and vaginal delivery: a detailed analysis to exclude the effects of medical disorders and other acute pre-existing physiological disturbances. Br J Obstet Gynaecol. 1990;97(10):883–92. - PubMed
-
- Ryding EL, Wijma K, Wijma B. Experiences of emergency cesarean section: A phenomenological study of 53 women. Birth. 1998;25(4):246–51. - PubMed
-
- Creedy DK, Shochet IM, Horsfall J. Childbirth and the development of acute trauma symptoms: incidence and contributing factors. Birth. 2000;27(2):104–11. - PubMed
-
- van Ham MA, van Dongen PW, Mulder J. Maternal consequences of caesarean section. A retrospective study of intraoperative and postoperative maternal complications of caesarean section during a 10-year period. Eur J Obstet Gynecol Reprod Biol. 1997;74(1):1–6. - PubMed
-
- Martin JA, Hamilton BE, Sutton PD, et al. Births: final data for 2002. Natl Vital Stat Rep. 2003;52(10):1–113. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
