

Training family physicians in shared decision-making to reduce the overuse of antibiotics in acute respiratory infections: a cluster randomized trial
- PMID: 22847969
- PMCID: PMC3447039
- DOI: 10.1503/cmaj.120568
Training family physicians in shared decision-making to reduce the overuse of antibiotics in acute respiratory infections: a cluster randomized trial
Abstract
Background: Few interventions have proven effective in reducing the overuse of antibiotics for acute respiratory infections. We evaluated the effect of DECISION+2, a shared decision-making training program, on the percentage of patients who decided to take antibiotics after consultation with a physician or resident.
Methods: We performed a randomized trial, clustered at the level of family practice teaching unit, with 2 study arms: DECISION+2 and control. The DECISION+2 training program included a 2-hour online tutorial followed by a 2-hour interactive seminar about shared decision-making. The primary outcome was the proportion of patients who decided to use antibiotics immediately after consultation. We also recorded patients' perception that shared decision-making had occurred. Two weeks after the initial consultation, we assessed patients' adherence to the decision, repeat consultation, decisional regret and quality of life.
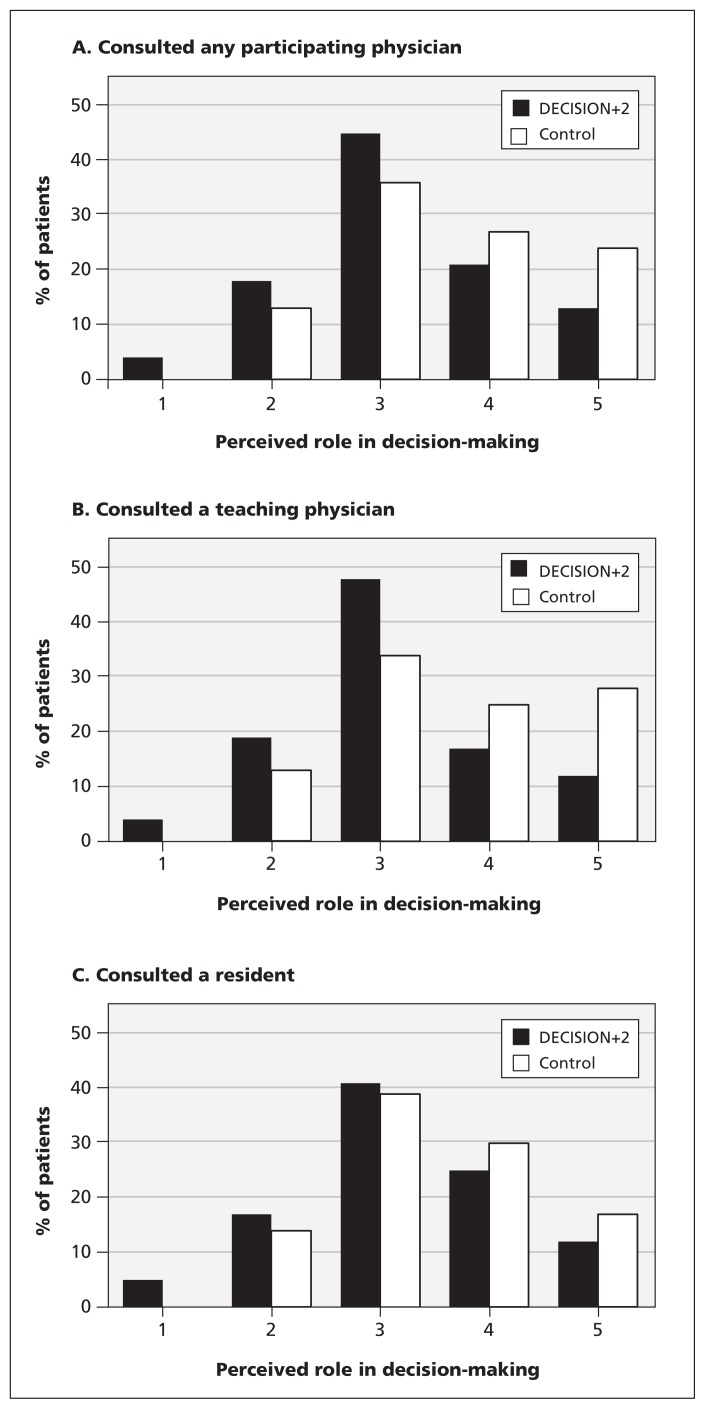
Results: We compared outcomes among 181 patients who consulted 77 physicians in 5 family practice teaching units in the DECISION+2 group, and 178 patients who consulted 72 physicians in 4 family practice teaching units in the control group. The percentage of patients who decided to use antibiotics after consultation was 52.2% in the control group and 27.2% in the DECISION+2 group (absolute difference 25.0%, adjusted relative risk 0.48, 95% confidence interval 0.34-0.68). DECISION+2 was associated with patients taking a more active role in decision-making (Z = 3.9, p < 0.001). Patient outcomes 2 weeks after consultation were similar in both groups.
Interpretation: The shared decision-making program DECISION+2 enhanced patient participation in decision-making and led to fewer patients deciding to use antibiotics for acute respiratory infections. This reduction did not have a negative effect on patient outcomes 2 weeks after consultation. ClinicalTrials.gov trial register no. NCT01116076.
Figures

References
-
- Coco A, Vernacchio L, Horst M, et al. Management of acute otitis media after publication of the 2004 AAP and AAFP clinical practice guideline. Pediatrics 2010;125:214–20 - PubMed
-
- Alberta Clinical Practice Guideline Working Group Guideline for the diagnosis and treatment of acute pharyngitis. Edmonton (AB): Alberta Clinical Practice Guidelines Program; 1999
-
- Agency for Healthcare Research and Quality (AHRQ) Update on acute bacterial rhinosinusitis. Rockville (MD): US Department of Health and Human Services; 2005
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical